Early terminated PEP RCT comparing HCQ and vitamin C with 781 low-risk patients (83% household contacts), reporting no significant differences.
Different results were reported at IDWeek from the AIM results.
The study enrolled people with their last exposure within 4 days, i.e., if someone was exposed for 30 days in a row, they could be enrolled anywhere from day 1 to day 34. Therefore many were likely infected earlier than the enrollment date. Note that PCR has a very high false negative rates, e.g., 100% on day 1 and 67% on day 4 here
ncbi.nlm.nih.gov.
50% of infections were detected by day 4. With the PCR false negatives and treatment delays it is likely that a majority of infections happened before enrollment or before HCQ can reach therapeutic levels.
Significantly more cases were caught at baseline in the control group (54 vs. 29 for HCQ) and excluded from analysis.
The early presentation stated that therapy started one day after enrollment and study supplies were sent to the participant "either by courier or mail". The published paper changes this to "courier delivery within 48 hours".
Overall delays are unclear but may be:
time since first exposure - unlimited
time from last exposure to enrollment - 10% reported as >= 5 days
time to telehealth meeting - 1 day (3 days if Friday enrollment?)
time to receive medication - <48 hours (including weekends?)
Symptomatic in this study was based on CDC-defined symptoms which contain symptoms that may be due to HCQ side effects.
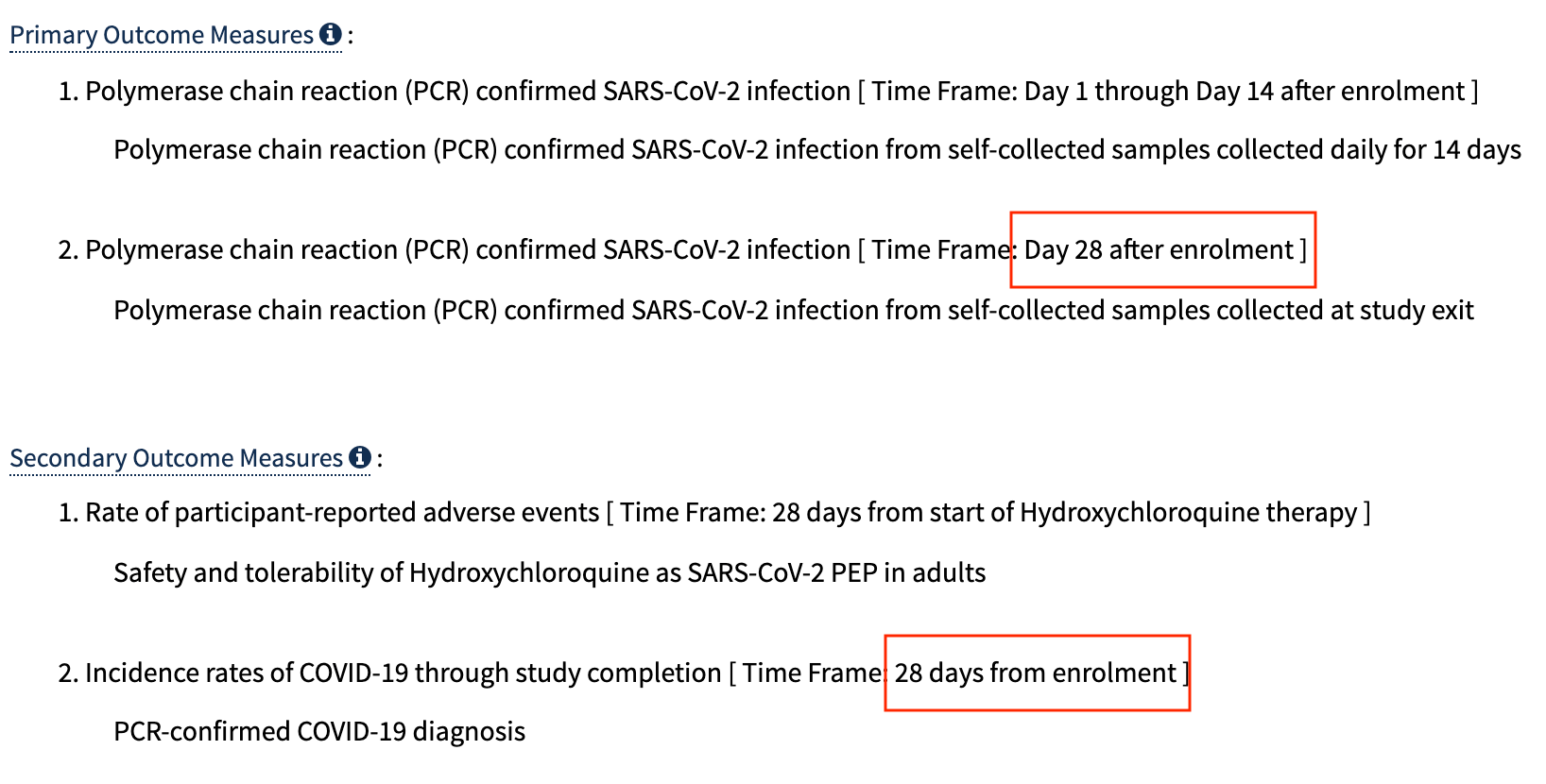
Some results have not been reported, including symptomatic @28 days. The study uses a low dosage over an extended period, therapeutic levels may only be reached nearer to day 14, if at all, so day 28 results should be more informative when available (although labeled a PEP trial, with the low dosage and continuous exposure for most participants it is more of a PrEP/PEP trial where benefit might be seen later as HCQ levels increase).
Endpoints were:
Primary outcomes:
PCR+ @28 days mITT - aHR 1.16 [0.77-1.73]
PCR+ @14 days mITT - aHR 1.10 [0.73-1.66] IDWeek report was different: aHR 0.99 [0.64-1.52]
PCR+ @14 days ITT - aHR 0.81 [0.57-1.14]
Secondary outcomes:
PCR+ symptomatic @28 days - NOT REPORTED YET
duration of shedding - NOT REPORTED YET
Not in study protocol:
PCR+ cumulative symptomatic @14 days - aHR 1.23 [0.76-1.99].
Dose in first 24 hours - 0.8g (compare with Boulware et al. 2g)
Dose in first 5 days - 1.6g (compare with Boulware et al. 3.8g)
Other research suggests vitamin C may be beneficial for COVID-19, e.g.
researchsquare.com. No information on severity of cases is provided. Binary PCR does not distinguish replication-competence. There were 2 COVID-19 hospitalizations, one in each group. Side effects were similar for HCQ and placebo. 83% medication adherence at day 14.
|
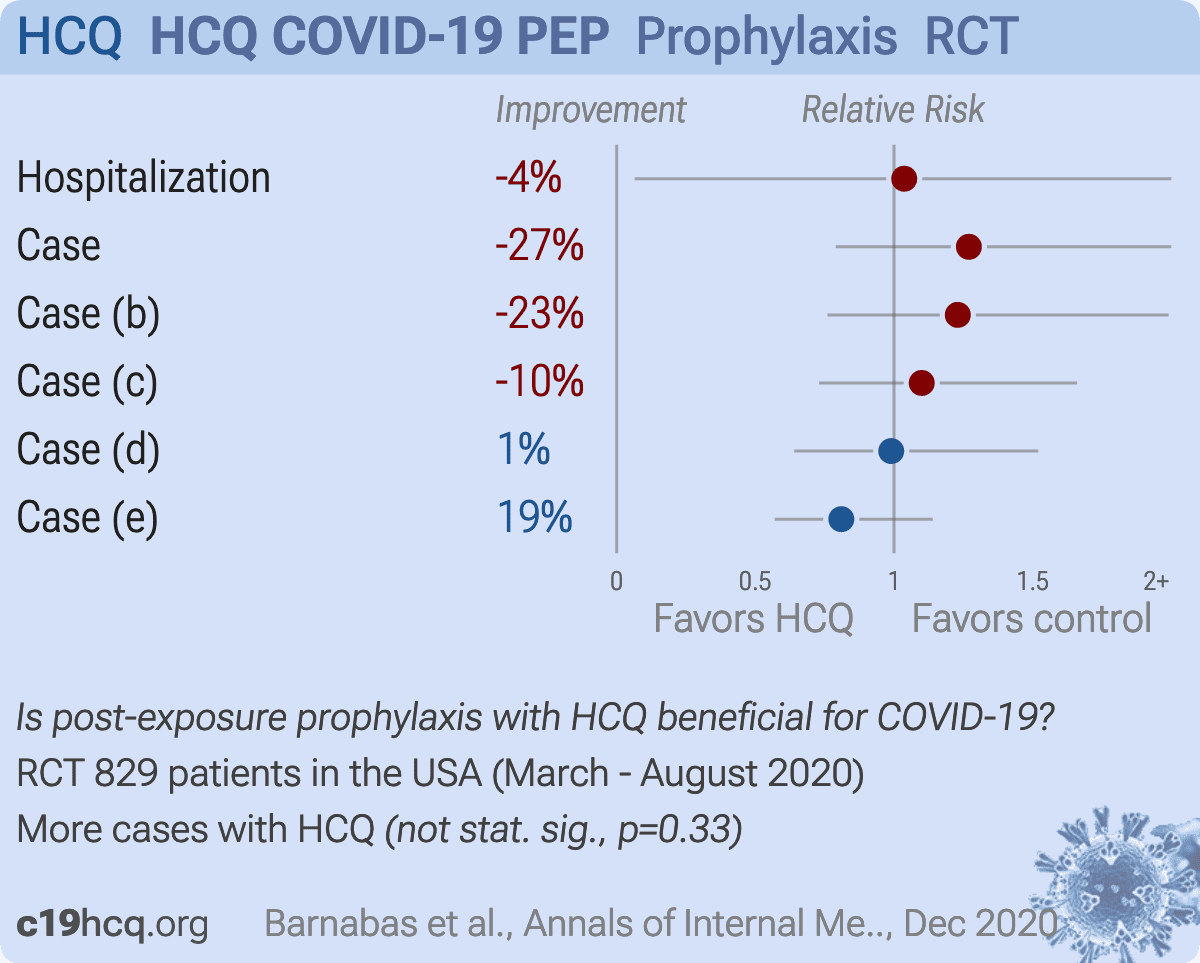
risk of hospitalization, 3.7% higher, RR 1.04, p = 1.00, treatment 1 of 407 (0.2%), control 1 of 422 (0.2%).
|
|
risk of case, 27.0% higher, HR 1.27, p = 0.33, treatment 43 of 353 (12.2%), control 33 of 336 (9.8%), adjusted per study, day 14 symptomatic mITT PCR+ AIM.
|
|
risk of case, 23.0% higher, HR 1.23, p = 0.41, treatment 40 of 317 (12.6%), control 32 of 309 (10.4%), adjusted per study, day 14 symptomatic mITT PCR+ IDWeek.
|
|
risk of case, 10.0% higher, HR 1.10, p = 0.66, treatment 53 of 353 (15.0%), control 45 of 336 (13.4%), adjusted per study, day 14 PCR+ mITT AIM.
|
|
risk of case, 1.0% lower, HR 0.99, p = 0.97, treatment 46 of 317 (14.5%), control 43 of 309 (13.9%), adjusted per study, day 14 PCR+ mITT IDWeek.
|
|
risk of case, 19.0% lower, HR 0.81, p = 0.23, treatment 82 of 387 (21.2%), control 99 of 393 (25.2%), NNT 25, adjusted per study, day 14 PCR+ ITT AIM.
|
|
Effect extraction follows pre-specified rules prioritizing more serious outcomes. Submit updates
|
Barnabas et al., 7 Dec 2020, Randomized Controlled Trial, USA, peer-reviewed, 30 authors, study period 31 March, 2020 - 21 August, 2020, trial
NCT04328961 (history) (HCQ COVID-19 PEP).
Hydroxychloroquine as Postexposure Prophylaxis to Prevent Severe Acute Respiratory Syndrome Coronavirus 2 Infection
MBChB, MSc, DPhil Ruanne V Barnabas, ScD Elizabeth R Brown, PhD Anna Bershteyn, MD Helen C Stankiewicz Karita, MD, MPH Christine Johnston, PhD, MPH Lorna E Thorpe, MD Angelica Kottkamp, MD, MPH Kathleen M Neuzil, MD, MPH Miriam K Laufer, MD Meagan Deming, PhD Michael K Paasche-Orlow, MD Patricia J Kissinger, PhD, MPH Alfred Luk, MD Kristopher Paolino, MD Raphael J Landovitz, MD, MSc Risa Hoffman, MD Torin T Schaafsma, MS Meighan L Krows, BA Katherine K Thomas, MS Susan Morrison, MD, MPH Harald S Haugen, MS Lara Kidoguchi, MPH Mark Wener, MD Alexander L Greninger, PhD, MS, MPhil Meei-Li Huang, PhD Keith R Jerome, MD, PhD; Anna Wald, MD, MPH Connie Celum, MD, MPH Helen Y Chu, MD, MPH Jared M Baeten
Annals of Internal Medicine, doi:10.7326/m20-6519
Background: Effective prevention against coronavirus disease 2019 (COVID-19), caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), is currently limited to nonpharmaceutical strategies. Laboratory and observational data suggested that hydroxychloroquine had biological activity against SARS-CoV-2, potentially permitting its use for prevention.
Objective: To test hydroxychloroquine as postexposure prophylaxis for SARS-CoV-2 infection. Design: Household-randomized, double-blind, controlled trial of hydroxychloroquine postexposure prophylaxis. (ClinicalTrials .gov: NCT04328961) Setting: National U.S. multicenter study. Participants: Close contacts recently exposed (<96 hours) to persons with diagnosed SARS-CoV-2 infection. Intervention: Hydroxychloroquine (400 mg/d for 3 days followed by 200 mg/d for 11 days) or ascorbic acid (500 mg/d followed by 250 mg/d) as a placebo-equivalent control. Measurements: Participants self-collected mid-turbinate swabs daily (days 1 to 14) for SARS-CoV-2 polymerase chain reaction (PCR) testing. The primary outcome was PCRconfirmed incident SARS-CoV-2 infection among persons who were SARS-CoV-2 negative at enrollment.
Results: Between March and August 2020, 671 households were randomly assigned: 337 (407 participants) to the hydroxychloroquine group and 334 (422 participants) to the control group. Retention at day 14 was 91%, and 10 724 of 11 606 (92%) expected swabs were tested. Among the 689 (89%) participants who were SARS-CoV-2 negative at baseline, there was no difference between the hydroxychloroquine and control groups in SARS-CoV-2 acquisition by day 14 (53 versus 45 events; adjusted hazard ratio, 1.10 [95% CI, 0.73 to 1.66]; P > 0.20). The frequency of participants experiencing adverse events was higher in the hydroxychloroquine group than the control group (66 [16.2%] versus 46 [10.9%], respectively; P = 0.026).
Limitation: The delay between exposure, and then baseline testing and the first dose of hydroxychloroquine or ascorbic acid, was a median of 2 days.
Conclusion: This rigorous randomized controlled trial among persons with recent exposure excluded a clinically meaningful effect of hydroxychloroquine as postexposure prophylaxis to prevent SARS-CoV-2 infection.
Corresponding Author: Ruanne V. Barnabas
References
Abella, Jolkovsky, Biney, the Prevention and Treatment of COVID-19 With Hydroxychloroquine (PATCH) Investigators. Efficacy and safety of hydroxychloroquine vs placebo for pre-exposure SARS-CoV-2 prophylaxis among health care workers: a randomized clinical trial, JAMA Intern Med,
doi:10.1001/jamainternmed.2020.6319Barnabas, Brown, Bershteyn, Hydroxychloroquine COVID-19 PEP Study Team. Efficacy of hydroxychloroquine for post-exposure prophylaxis to prevent severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection among adults exposed to coronavirus disease (COVID-19): a structured summary of a study protocol for a randomised controlled trial [Letter, Trials,
doi:10.1186/s13063-020-04446-4Baum, Fulton, Wloga, Antibody cocktail to SARS-CoV-2 spike protein prevents rapid mutational escape seen with individual antibodies, Science,
doi:10.1126/science.abd0831Boulware, Pullen, Bangdiwala, A randomized trial of hydroxychloroquine as postexposure prophylaxis for covid-19, N Engl J Med,
doi:10.1056/NEJMoa2016638Cancer, None
Celum, Chu, Baeten, Laufer, Kissinger et al., Critical revision for important intellectual content
Conte, None
Dong, Du, Gardner, An interactive web-based dashboard to track COVID-19 in real time
Drake, Docherty, Weiser, The effects of physical distancing on population mobility during the COVID-19 pandemic in the UK, Lancet Digit Health,
doi:10.1016/S2589-7500(20)30134-5Drs, Barnabas, Karita, Morrison, Baeten; Mr et al., Kidoguchi: International Clinical Research Center (ICRC)
Ferreira, Oliveira, Silva, Bettencourt, Chronic treatment with hydroxychloroquine and SARS-CoV-2 infection, J Med Virol,
doi:10.1002/jmv.26286Gentile, Maraolo, Piscitelli, COVID-19: time for post-exposure prophylaxis, Int J Environ Res Public Health
Hoffmann, Mösbauer, Hofmann-Winkler, Chloroquine does not inhibit infection of human lung cells with SARS-CoV-2, Nature,
doi:10.1038/s41586-020-2575-3Ikematsu, Hayden, Kawaguchi, Baloxavir marboxil for prophylaxis against influenza in household contacts, N Engl J Med,
doi:10.1056/NEJMoa1915341Lee, Son, Peck, Can post-exposure prophylaxis for COVID-19 be considered as an outbreak response strategy in longterm care hospitals, Int J Antimicrob Agents,
doi:10.1016/j.ijantimicag.2020.105988Lieberman, Pepper, Naccache, Comparison of commercially available and laboratory-developed assays for in vitro detection of SARS-CoV-2 in clinical laboratories, J Clin Microbiol,
doi:10.1128/JCM.00821-20Madewell, Yang, Longini, Household transmission of SARS-CoV-2: a systematic review and meta-analysis of secondary attack rate,
doi:10.1101/2020.07.29.20164590Mitja, Ubals, Corbacho, A cluster-randomized trial of hydroxychloroquine as prevention of Covid-19 transmission and disease. medRxiv,
doi:10.1101/2020.07.20.20157651Mitjà, Clotet, Use of antiviral drugs to reduce COVID-19 transmission
North, Seattle, Wa ; Dr, Bershteyn: Translational Research Building, 227 East 30th
O'brien, Fleming, A multiple testing procedure for clinical trials, Biometrics
Oran, Topol, Prevalence of asymptomatic SARS-CoV-2 infection. A narrative review, Ann Intern Med,
doi:10.7326/M20-3012Perera, Tso, Tsang, SARS-CoV-2 virus culture and subgenomic RNA for respiratory specimens from patients with mild coronavirus disease, Emerg Infect Dis,
doi:10.3201/eid2611.20321930Rolain, Colson, Raoult, Recycling of chloroquine and its hydroxyl analogue to face bacterial, fungal and viral infections in the 21st century, Int J Antimicrob Agents
Therneau, Grambsch, Modeling Survival Data: Extending the Cox Model
Wang, Cao, Zhang, Remdesivir and chloroquine effectively inhibit the recently emerged novel coronavirus (2019-nCoV)
Welliver, Monto, Carewicz, Oseltamivir Post Exposure Prophylaxis Investigator Group. Effectiveness of oseltamivir in preventing influenza in household contacts: a randomized controlled trial, JAMA
Wu, Mcgoogan, Characteristics of and important lessons from the coronavirus disease 2019 (COVID-19) outbreak in China: summary of a report of 72?314 cases from the Chinese Center for Disease Control and Prevention, JAMA,
doi:10.1001/jama.2020.2648Yao, Ye, Zhang, In vitro antiviral activity and projection of optimized dosing design of hydroxychloroquine for the treatment of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), Clin Infect Dis,
doi:10.1093/cid/ciaa237

{kind=link}
{kind=link}