CPAP Treatment In COVID-19 Patients: A Retrospective Observational Study In The Emergency Department
Nicolò Capsoni, Daniele Privitera, Annamaria Mazzone, Chiara Airoldi, Valentina Albertini, Laura Angaroni, Marta Bergamaschi, Alberto Dal Molin, Elisa Forni, Federico Pierotti, Eugenia Rocca, Fabrizio Vincenti, Andrea Bellone
doi:10.21203/rs.3.rs-113418/v1
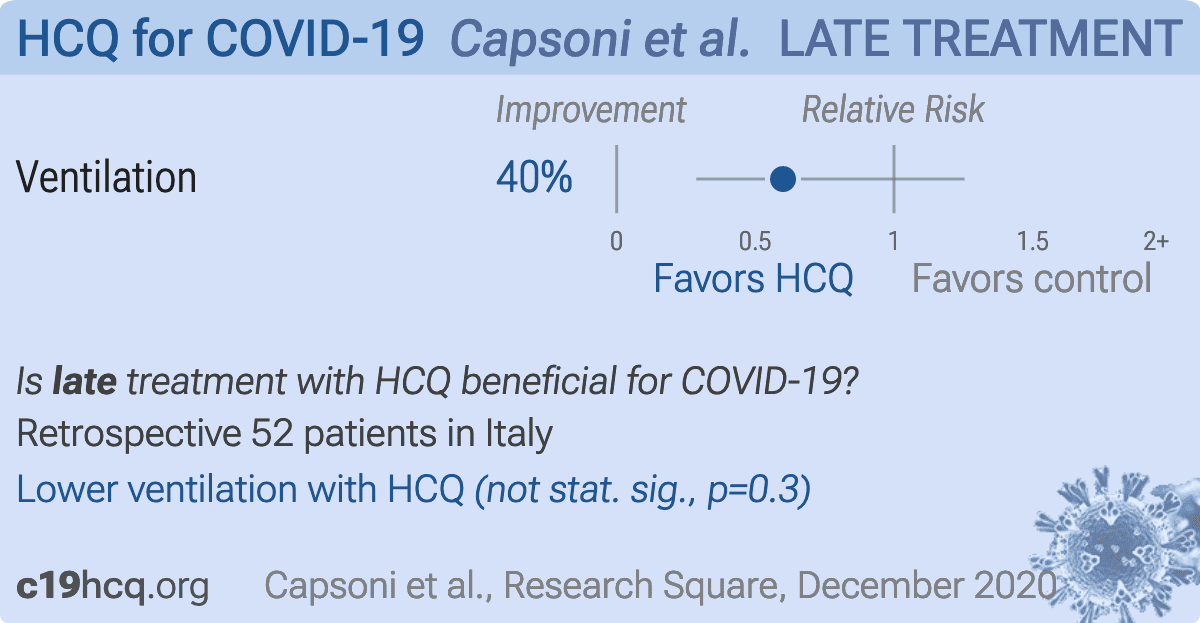
Background During COVID-19 outbreak, with the increasing number of patients presenting with acute respiratory failure (ARF), a large use of non-invasive positive pressure ventilation (NIPPV) was done in the Emergency Departments (EDs) and medical wards despite the lack of recommendations. We aimed to assess the use of continuous positive airway pressure (CPAP) in the ED. The primary endpoint was the rate of CPAP failure and the need of endotracheal intubation (ETI). Secondary endpoints were in-hospital mortality and intensive care unit (ICU) and in-hospital length of stay.
Methods A retrospective observational study enrolling adult patients admitted to the ED of Niguarda Hospital, Milan, Italy, with ARF due to COVID-19 pneumonia from March 18th to April 18th 2020, was conducted. Only patients who strictly followed a local CPAP protocol were enrolled.
Results A total of 52 patients were included in this study. 38 patients (73%) were judged eligible for ETI. 18 (34.6%) were intubated. 16 (30.8%) patients died: 7 (38.9%) and 9 (26.5%) in the ETI and non-ETI group respectively. The median hospital length of stay was different in ETI and non-ETI patients: 26 days [IQR 16-37] vs 15 days [IQR 9-17] (p = 0.005). The median invasive mechanical ventilation time was 11 days [IQR 7-21] with an ICU length of stay of 14.5 days [IQR 10-28]. During the CPAP trial, variations between ETI and non-ETI patients over time were found for positive end-expiratory pressure (PEEP) (p = 0.003) and respiratory rate (RR) (p = 0.059). Conclusionss A short closed monitored CPAP trial could be considered for ARF due to COVID-19 pneumonia before considering ETI. A progressive PEEP titration should target patient's RR reduction. More studies are needed to evaluate the e cacy and predictors of failure of CPAP and NIPPV in patients with ARF due to COVID-19 pneumonia.
References
Arabi, Fowler, Hayden, Critical care management of adults with community-acquired severe respiratory viral infection, Intensive Care Med,
doi:10.1007/s00134-020-05943-5Chung, Bernheim, Mei, Zhang, Huang et al., CT imaging features of 2019 novel coronavirus (2019-NCoV), Radiology
Elm, Altman, Egger, Pocock, Gøtzsche et al., The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: Guidelines for reporting observational studies, Bull World Health Organ
Gattinoni, Chiumello, Caironi, Busana, Romitti et al., COVID-19 pneumonia: different respiratory treatments for different phenotypes?, Intensive Care Med,
doi:10.1007/s00134-020-06033-2Gattinoni, Chiumello, Rossi, Rochwerg, Brochard et al., O cial ERS/ATS clinical practice guidelines: Noninvasive ventilation for acute respiratory failure, Eur Respir J,
doi:10.1183/13993003.02426-2016Grasselli, Zangrillo, Zanella, Antonelli, Cabrini et al., Baseline Characteristics and Outcomes of 1591 Patients Infected with SARS-CoV-2 Admitted to ICUs of the Lombardy Region, Italy, JAMA -J Am Med Assoc
Kelly, Matthay, Prevalence and severity of neurologic dysfunction in critically ill patients: In uence on need for continued mechanical ventilation, Chest,
doi:10.1378/chest.104.6.1818Masclans, Pérez, Almirall, Lorente, Marqués et al., Early non-invasive ventilation treatment for severe in uenza pneumonia, Clin Microbiol Infect
Navalesi, Maggiore, Positive end-expiratory pressure
Nicolini, Tonveronachi, Navalesi, Antonelli, Valentini et al., Effectiveness and predictors of success of noninvasive ventilation during H1N1 pandemics: A multicenter study, Minerva Anestesiol
Privitera, Angaroni, Capsoni, Forni, Pierotti et al., Flowchart for non-invasive ventilation support in COVID-19 patients from a northern Italy Emergency Department, Intern Emerg,
doi:10.1007/s11739-020-02370-8Radovanovic, Rizzi, Pini, Saad, Chiumello et al., Helmet CPAP to Treat Acute Hypoxemic Respiratory Failure in Patients with COVID-19: A Management Strategy Proposal, J Clin Med
Respiratory Rate, Peep, con dence intervals obtained performing mixed models, which take into account for repeated measures within subjects
Rodríguez, Ferri, Loeches, Díaz, Masclans et al., Risk factors for noninvasive ventilation failure in critically ill subjects with con rmed in uenza infection, Respir Care
Verity, Okell, Dorigatti, Winskill, Whittaker et al., Estimates of the severity of coronavirus disease 2019: a model-based analysis, Lancet Infect Dis
Zhou, Yu, Du, Fan, Liu et al., Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: a retrospective cohort study, Lancet,
doi:10.1016/S0140-6736(20)30566-3


{kind=link}