Small study of SLE patients taking HCQ with a phone survey for COVID-19 suggestive symptoms. There was 2 hospitalizations (group not identified) and no ICU or death cases. A similar percentage of suspected infections were reported for HCQ users and non-HCQ users, RR 0.96, p = 0.93.
There was no mortality and severity was not analyzed to determine if HCQ treated patients fared better. No adjustment for concomitant medications or severity of SLE. Only 5 cases were PCR confirmed.
This study is excluded in the after exclusion results of meta
analysis:
not fully adjusting for the baseline risk differences within systemic autoimmune patients.
|
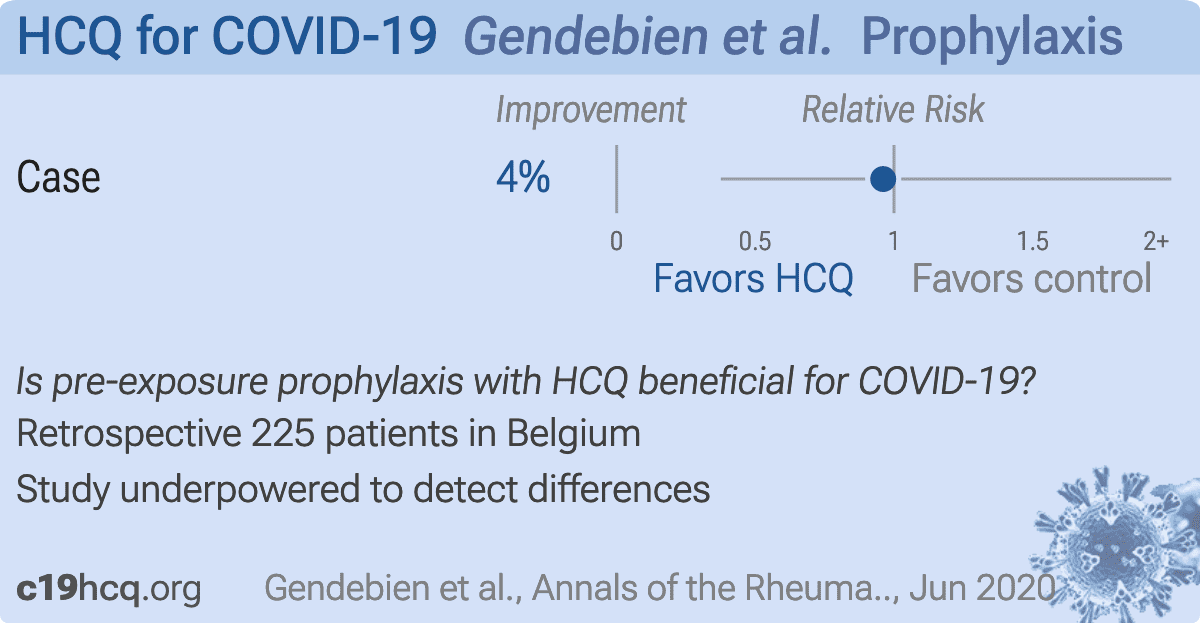
risk of case, 3.9% lower, RR 0.96, p = 0.93, treatment 12 of 152 (7.9%), control 6 of 73 (8.2%), NNT 308.
|
|
Effect extraction follows pre-specified rules prioritizing more serious outcomes. Submit updates
|
Gendebien et al., 25 Jun 2020, retrospective, Belgium, peer-reviewed, survey, 9 authors.
Systematic analysis of COVID-19 infection and symptoms in a systemic lupus erythematosus population: correlation with disease characteristics, hydroxychloroquine use and immunosuppressive treatments
Zoé Gendebien, Christian Von Frenckell, Clio Ribbens, Béatrice André, Marie Thys, Marjorie Gangolf, Laurence Seidel, Michel G Malaise, Dr Olivier Malaise
Annals of the Rheumatic Diseases, doi:10.1136/annrheumdis-2020-218244
We read with interest the article of Bozzalla Cassione et al about COVID-19 incidence in their systemic lupus erythematosus (SLE) cohort. 1 Their study adds useful epidemiological information about COVID-19 risk in SLE. 1 They suggest that hydroxycholoroquine was not protective, but could not draw definite conclusion and open the question to immunosuppressive drugs' influence. We would like to share analysis of our SLE cohort (n=225) that can help to answer these questions and determine COVID-19 infection risk factors. Determining COVID-19 incidence is challenging: PCR lacks sensitivity, was usually realised only in severely ill patients and patients with suggestive benign symptoms could stay at home without medical contact. We studied the incidence of COVID-19 infection, either asserted or suspected, by analysing positive nasopharyngeal PCR, hospitalisation or contact with emergency department, but also suspected diagnosis in ambulatory medicine. Each patient was called by phone to determine COVID-19 suggestive symptoms since 4 February 2020, date of the first case in our country. Among our patients, 92.9% were female, with a mean (±SD) age of 51.7 (±14.9) years. Most recent biological evaluation showed positivity for ds-DNA in 24% (median (min-max) levels: 139 (12-758) IU/mL). Mean (±SD) number of 1997 American College of Rheumatology (ACR), 2019 American College of Rheumatology/European League Against Rheumatism (ACR/ EULAR) and Systemic Lupus International Collaborating Clinics (SLICC) classification criteria were 4.5 (±1.5), 20.0 (±8.1) and 5.8 (±2.2), respectively. One hundred and fifty-two (68.1%) patients received chronic treatment with hydroxychloroquine,
References
Bozzalla Cassione, Zanframundo, Biglia, COVID-19 infection in a northern-Italian cohort of systemic lupus erythematosus assessed by telemedicine, Ann Rheum Dis,
doi:10.1136/annrheumdis-2020-217717Gianfrancesco, Hyrich, Al-Adely, Characteristics associated with hospitalisation for COVID-19 in people with rheumatic disease: data from the COVID-19 global rheumatology alliance physician-reported registry, Ann Rheum Dis,
doi:10.1136/annrheumdis-2020-217871Haberman, Axelrad, Chen, Covid-19 in Immune-Mediated Inflammatory Diseases -Case Series from New York, N Engl J Med,
doi:10.1056/NEJMc2009567Mathian, Mahevas, Rohmer, Clinical course of coronavirus disease 2019 (COVID-19) in a series of 17 patients with systemic lupus erythematosus under longterm treatment with hydroxychloroquine, Ann Rheum Dis,
doi:10.1136/annrheumdis-2020-217566Xu, Chen, Yuan, Factors associated with prolonged viral RNA shedding in patients with COVID-19, Clinical Infectious Diseases

{kind=link}
{kind=link}