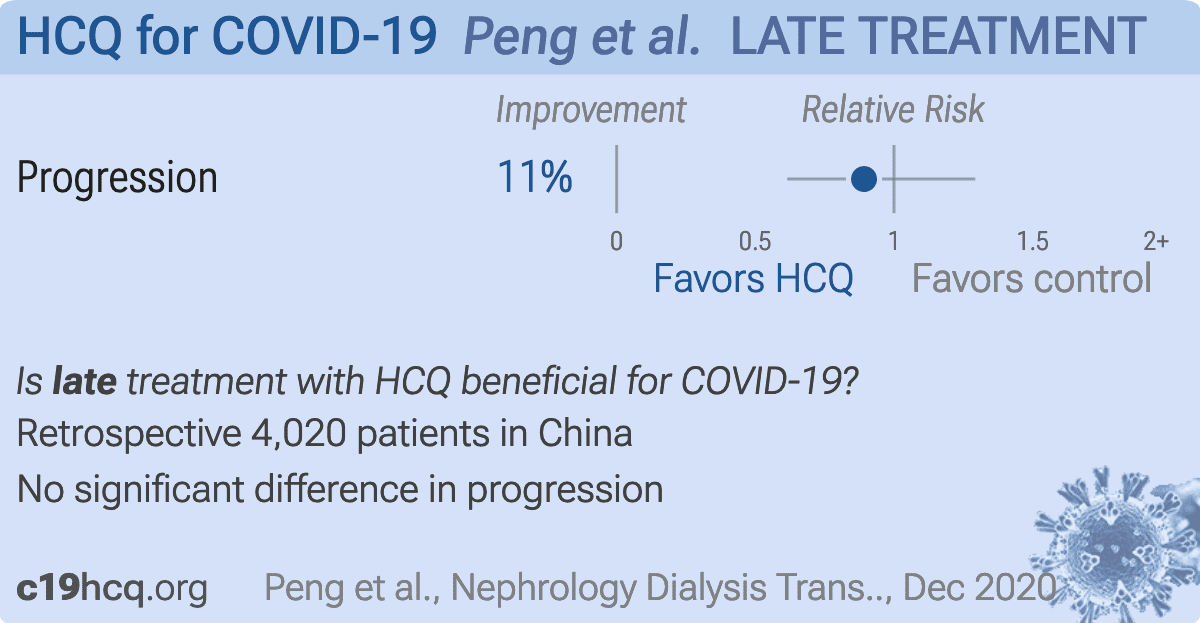
Early versus late acute kidney injury among patients with COVID-19—a multicenter study from Wuhan, China
Suyuan Peng, Huai-Yu Wang, Xiaoyu Sun, Pengfei Li, Zhanghui Ye, Qing Li, Jinwei Wang, Xuanyu Shi, Liu Liu, Ying Yao, Rui Zeng, Fan He, Junhua Li, Shuwang Ge, Xianjun Ke, Zhibin Zhou, Erdan Dong, Haibo Wang, Gang Xu, Luxia Zhang, Ming-Hui Zhao
Nephrology Dialysis Transplantation, doi:10.1093/ndt/gfaa288
Background. Acute kidney injury (AKI) is an important complication of coronavirus disease 2019 , which could be caused by both systematic responses from multi-organ dysfunction and direct virus infection. While advanced evidence is needed regarding its clinical features and mechanisms. We aimed to describe two phenotypes of AKI as well as their risk factors and the association with mortality. Methods. Consecutive hospitalized patients with COVID-19 in tertiary hospitals in Wuhan, China from 1 January 2020 to 23 March 2020 were included. Patients with AKI were classified as AKI-early and AKI-late according to the sequence of organ dysfunction (kidney as the first dysfunctional organ or not). Demographic and clinical features were compared between two AKI groups. Their risk factors and the associations with inhospital mortality were analyzed. Results. A total of 4020 cases with laboratory-confirmed COVID-19 were included and 285 (7.09%) of them were identified as AKI. Compared with patients with AKI-early, patients with AKI-late had significantly higher levels of systemic inflammatory markers. Both AKIs were associated with an increased risk of in-hospital mortality, with similar fully adjusted hazard ratios of 2.46 [95% confidence interval (CI) 1.35-4.49] for AKIearly and 3.09 (95% CI 2.17-4.40) for AKI-late. Only hypertension was independently associated with the risk of AKI-early. While age, history of chronic kidney disease and the levels of inflammatory biomarkers were associated with the risk of AKIlate. Conclusions. AKI among patients with COVID-19 has two clinical phenotypes, which could be due to different mechanisms. Considering the increased risk for mortality for both phenotypes, monitoring for AKI should be emphasized during COVID-19.
References
Akram, Singanayagam, Choudhury, Incidence and prognostic implications of acute kidney injury on admission in patients with community-acquired pneumonia, Chest
Ali, Daoud, Mohamed, Survival rate in acute kidney injury superimposed COVID-19 patients: a systematic review and meta-analysis, Ren Fail
Arentz, Yim, Klaff, Characteristics and outcomes of 21 critically ill patients with COVID-19 in Washington State, JAMA
Batlle, Soler, Sparks, Acute kidney injury in COVID-19: emerging evidence of a distinct pathophysiology, J Am Soc Nephrol
Bhatia, Moochhala, Role of inflammatory mediators in the pathophysiology of acute respiratory distress syndrome, J Pathol
Braun, Lutgehetmann, Pfefferle, SARS-CoV-2 renal tropism associates with acute kidney injury, Lancet
Calomeni, Satoskar, Ayoub, Multivesicular bodies mimicking SARS-CoV-2 in patients without COVID-19, Kidney Int
Chan, Chaudhary, Saha, AKI in hospitalized patients with COVID-19, J Am Soc Nephrol
Chen, Shao, Hsu, Incidence of acute kidney injury in COVID-19 infection: a systematic review and meta-analysis, Crit Care
Chen, Wu, Chen, Clinical characteristics of 113 deceased patients with coronavirus disease 2019: retrospective study, BMJ
Cheng, Luo, Wang, Kidney disease is associated with in-hospital death of patients with COVID-19, Kidney Int
Chu, Tsang, Tang, Acute renal impairment in coronavirus-associated severe acute respiratory syndrome, Kidney Int
Domenech, Perez, Saldarini, Kidney-lung pathophysiological crosstalk: its characteristics and importance, Int Urol Nephrol
Farkash, Wilson, Jentzen, Ultrastructural evidence for direct renal infection with SARS-CoV-2, J Am Soc Nephrol
Friedman, Pollak, APOL1 and kidney disease: from genetics to biology, Annu Rev Physiol
Goldsmith, Miller, Martines, Electron microscopy of SARS-CoV-2: a challenging task, Lancet
Guan, Ni, Hu, Clinical characteristics of coronavirus disease 2019 in China, N Engl J Med
Gupta, Madhavan, Sehgal, Extrapulmonary manifestations of COVID-19, Nat Med
Hirsch, Ng, Ross, Acute kidney injury in patients hospitalized with COVID-19, Kidney Int
Huang, Su, An interferon-c-related cytokine storm in SARS patients, J Med Virol
James, Levey, Tonelli, Incidence and prognosis of acute kidney diseases and disorders using an integrated approach to laboratory measurements in a universal health care system, JAMA
Kissling, Rotman, Gerber, Collapsing glomerulopathy in a COVID-19 patient, Kidney Int
Kong, Chui, Lim, Elucidating the molecular physiopathology of acute respiratory distress syndrome in severe acute respiratory syndrome patients, Virus Res
Kudose, Batal, Santoriello, Kidney biopsy findings in patients with COVID-19, J Am Soc Nephrol
Li, Liu, Zhang, SARS-CoV-2 and viral sepsis: observations and hypotheses, Lancet
Li, Wu, Yao, Caution on kidney dysfunctions of COVID-19 patients, medRxiv
Merad, Martin, Pathological inflammation in patients with COVID-19: a key role for monocytes and macrophages, Nat Rev Immunol
Mohamed, Lukitsch, Torres-Ortiz, Acute kidney injury associated with coronavirus disease 2019 in urban New Orleans
Naicker, Yang, Hwang, The novel coronavirus 2019 epidemic and kidneys, Kidney Int
Ng, Nh, An empirical comparison of statistical tests for assessing the proportional hazards assumption of Cox's model, Stat Med
Polak, Van Gool, Cohen, A systematic review of pathological findings in COVID-19: a pathophysiological timeline and possible mechanisms of disease progression, Mod Pathol
Puelles, Lutgehetmann, Lindenmeyer, Multiorgan and renal tropism of SARS-CoV-2, N Engl J Med
Ronco, Bellomo, Kellum, Acute kidney injury, Lancet
Ronco, Reis, Kidney involvement in COVID-19 and rationale for extracorporeal therapies, Nat Rev Nephrol
Roufosse, Curtis, Moran, Electron microscopic investigations in COVID-19: not all crowns are coronas, Kidney Int
Sharma, Uppal, Wanchoo, COVID-19-associated kidney injury: a case series of kidney biopsy findings, J Am Soc Nephrol
Su, Yang, Renal histopathological analysis of 26 postmortem findings of patients with COVID-19 in China, Kidney Int
Wang, Hu, Hu, Clinical characteristics of 138 hospitalized patients with 2019 novel coronavirus-infected pneumonia in Wuhan, China, JAMA
Werion, Belkhir, Perrot, SARS-CoV-2 causes a specific dysfunction of the kidney proximal tubule, Kidney Int
Wu, Larsen, Hernandez-Arroyo, AKI and collapsing glomerulopathy associated with COVID-19 and APOL 1 high-risk genotype, J Am Soc Nephrol
Xu, Han, Li, Effective treatment of severe COVID-19 patients with tocilizumab, Proc Natl Acad Sci
Yang, Xing, Wang, Acute kidney injury in China: a crosssectional survey, Lancet
Yang, Yu, Xu, Clinical course and outcomes of critically ill patients with SARS-CoV-2 pneumonia in Wuhan, China: a single-centered, retrospective, observational study, Lancet Respir Med
Zhang, Zhao, Zuo, China Kidney Disease Network (CK-NET) 2015 annual data report, Kidney Int Suppl
Zhou, Yu, Du, Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: a retrospective cohort study, Lancet


{kind=link}