Hydroxychloroquine as Pre-exposure Prophylaxis for Coronavirus Disease 2019 (COVID-19) in Healthcare Workers: A Randomized Trial
Radha Rajasingham, Ananta S Bangdiwala, Melanie R Nicol, Caleb P Skipper, Katelyn A Pastick, Margaret L Axelrod, Matthew F Pullen, Alanna A Nascene, Darlisha A Williams, Nicole W Engen, Elizabeth C Okafor, Brian I Rini, Ingrid A Mayer, Emily G Mcdonald, Todd C Lee, Peter Li, Lauren J Mackenzie, Justin M Balko, Stephen J Dunlop, Katherine H Hullsiek, David R Boulware, Sarah M Lofgren, Mahsa Abassi, Andrew Balster, Lindsey B Collins, Glen Drobot, Douglas S Krakower, Sylvain A Lother, Dylan S Mackay, Cameron Meyer-Mueller, Stephen Selinsky, Dayna Solvason, Ryan Zarychanski, Rebecca Zash
Clinical Infectious Diseases, doi:10.1093/cid/ciaa1571
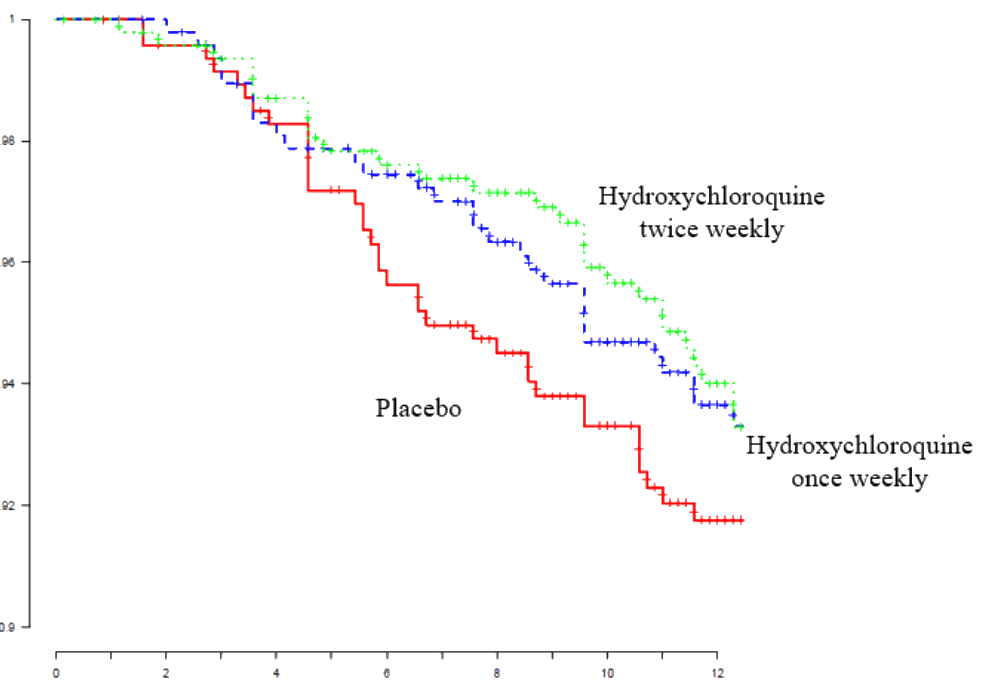
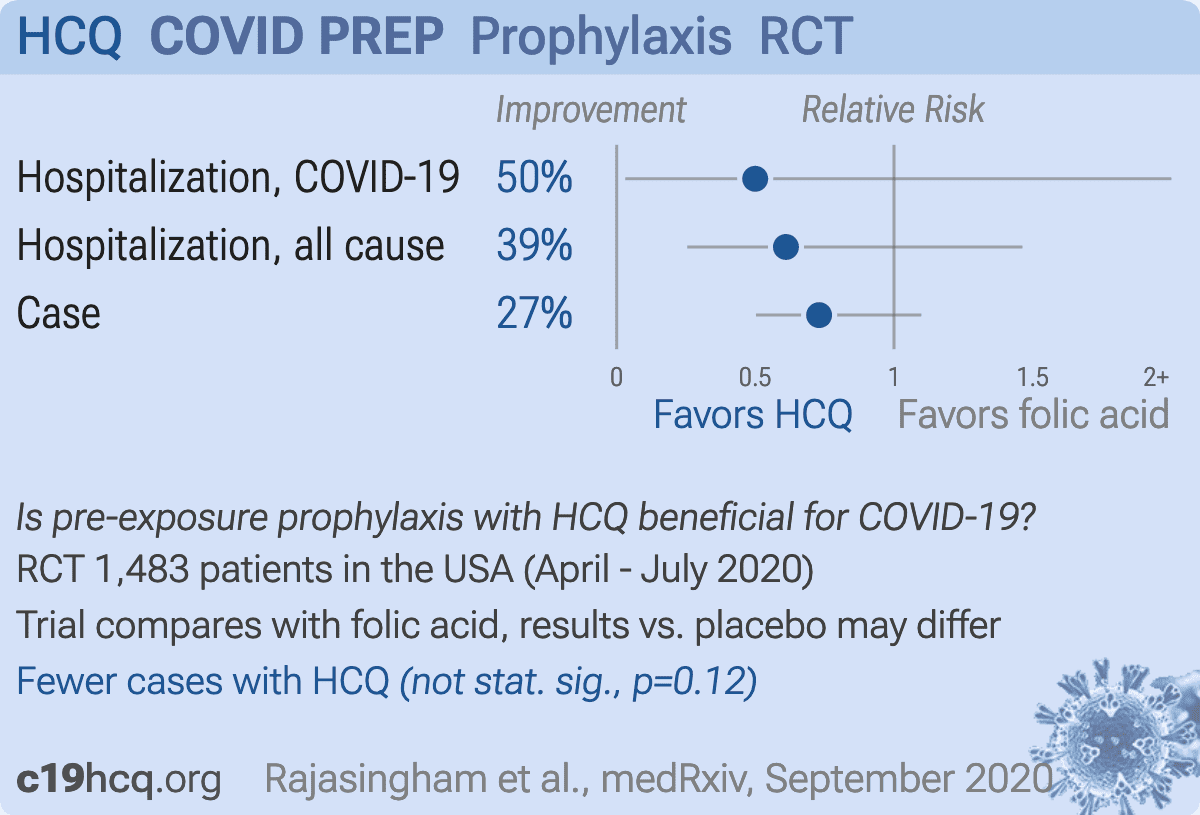
Background. Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) is a rapidly emerging virus causing the ongoing coronavirus disease 2019 (COVID-19) pandemic with no known effective prophylaxis. We investigated whether hydroxychloroquine could prevent SARS-CoV-2 in healthcare workers at high risk of exposure. Methods. We conducted a randomized, double-blind, placebo-controlled clinical trial of healthcare workers with ongoing exposure to persons with SARS-CoV-2, including those working in emergency departments, intensive care units, COVID-19 hospital wards, and first responders. Participants across the United States and in the Canadian province of Manitoba were randomized to hydroxychloroquine loading dose then 400 mg once or twice weekly for 12 weeks. The primary endpoint was confirmed or probable COVID-19-compatible illness. We measured hydroxychloroquine whole-blood concentrations. Results. We enrolled 1483 healthcare workers, of whom 79% reported performing aerosol-generating procedures. The incidence of COVID-19 (laboratory-confirmed or symptomatic compatible illness) was 0.27 events/person-year with once-weekly and 0.28 events/person-year with twice-weekly hydroxychloroquine compared with 0.38 events/person-year with placebo. For once-weekly hydroxychloroquine prophylaxis, the hazard ratio was .72 (95% CI, .44-1.16; P = .18) and for twice-weekly was .74 (95% CI, .46-1.19; P = .22) compared with placebo. Median hydroxychloroquine concentrations in whole blood were 98 ng/mL (IQR, 82-120) with onceweekly and 200 ng/mL (IQR, 159-258) with twice-weekly dosing. Hydroxychloroquine concentrations did not differ between participants who developed COVID-19-compatible illness (154 ng/mL) versus participants without COVID-19 (133 ng/mL; P = .08). Conclusions. Pre-exposure prophylaxis with hydroxychloroquine once or twice weekly did not significantly reduce laboratoryconfirmed COVID-19 or COVID-19-compatible illness among healthcare workers. clinical Trials Registration. NCT04328467.
Supplementary Data Supplementary materials are available at Clinical Infectious Diseases online. Consisting of data provided by the authors to benefit the reader, the posted materials are not copyedited and are the sole responsibility of the authors, so questions or comments should be addressed to the corresponding author.
Notes
References
Abella, Jolkovsky, Biney, Efficacy and safety of hydroxychloroquine vs placebo for pre-exposure SARS-CoV-2 prophylaxis among health care workers: a randomized clinical trial, JAMA Intern Med,
doi:10.1001/jamainternmed.2020.6319Al-Kofahi, Jacobson, Boulware, Finding the dose for hydroxychloroquine prophylaxis for COVID-19: the desperate search for effectiveness, Clin Pharmacol Ther,
doi:10.1002/cpt.1874Borba, Val, Sampaio, Effect of high vs low doses of chloroquine diphosphate as adjunctive therapy for patients hospitalized with severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection: a randomized clinical trial, JAMA Netw Open
Boulware, Pullen, Bangdiwala, A randomized trial of hydroxychloroquine as postexposure prophylaxis for Covid-19, N Engl J Med
Fan, Zhang, Liu, Connecting hydroxychloroquine in vitro antiviral activity to in vivo concentration for prediction of antiviral effect: a critical step in treating COVID-19 patients, Clin Infect Dis,
doi:10.1093/cid/ciaa623Harris, Taylor, Minor, The REDCap consortium: building an international community of software platform partners, J Biomed Inform
Kucirka, Lauer, Laeyendecker, Boon, Lessler, Variation in falsenegative rate of reverse transcriptase polymerase chain reaction-based SARS-CoV-2 tests by time since exposure, Ann Intern Med
Lancet, Expression of concern: hydroxychloroquine or chloroquine with or without a macrolide for treatment of COVID-19: a multinational registry analysis, Lancet
Lim, Im, Cho, Pharmacokinetics of hydroxychloroquine and its clinical implications in chemoprophylaxis against malaria caused by Plasmodium vivax, Antimicrob Agents Chemother
Liu, Cao, Xu, Hydroxychloroquine, a less toxic derivative of chloroquine, is effective in inhibiting SARS-CoV-2 infection in vitro, Cell Discov
Magagnoli, Narendran, Pereira, Outcomes of hydroxychloroquine usage in United States veterans hospitalized with Covid-19,
doi:10.1016/j.medj.2020.06.001Prevention, Interim, for healthcare personnel with potential exposure to COVID-19
Qu, Brady, Apilado, Capillary blood collected on volumetric absorptive microsampling (VAMS) device for monitoring hydroxychloroquine in rheumatoid arthritis patients, J Pharm Biomed Anal
Skipper, Pastick, Engen, Hydroxychloroquine in nonhospitalized adults with early COVID-19: a randomized trial, Ann Intern Med,
doi:10.7326/M20-4207Tett, Cutler, Day, Brown, A dose-ranging study of the pharmacokinetics of hydroxy-chloroquine following intravenous administration to healthy volunteers, Br J Clin Pharmacol
Vincent, Bergeron, Benjannet, Chloroquine is a potent inhibitor of SARS coronavirus infection and spread, Virol J
Wang, Cao, Zhang, Remdesivir and chloroquine effectively inhibit the recently emerged novel coronavirus (2019-nCoV) in vitro, Cell Res
Yao, Ye, Zhang, In vitro antiviral activity and projection of optimized dosing design of hydroxychloroquine for the treatment of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), Clin Infect Dis

{kind=link}
{kind=link}