COVID-19 was determined via PCR+ results, therefore authors include patients asymptomatic for COVID-19, but in the hospital for other reasons. While authors adjust for severity, the method used is very poor. 93.5% of patients are classified as "mild", which is patients with no documented care in a critical care unit within 8 hours of admission. Therefore almost all patients are in the same category, and those in a different category may be due to symptoms unrelated to COVID-19. Lower bias toward male patients in the control group also agrees with the hypothesis that the control group is made up of more people that were in hospital for another reason.
Since the analysis covers the initial period of the pandemic in the USA, it is likely that HCQ was used more often earlier in the analysis period when treatment protocols were considerably worse. It's unclear why the analysis only considers patients up to April 27, when the manuscript was submitted in October.
This study is excluded in the after exclusion results of meta
analysis:
includes PCR+ patients that may be asymptomatic for COVID-19 but in hospital for other reasons; substantial unadjusted
confounding by indication likely.
|
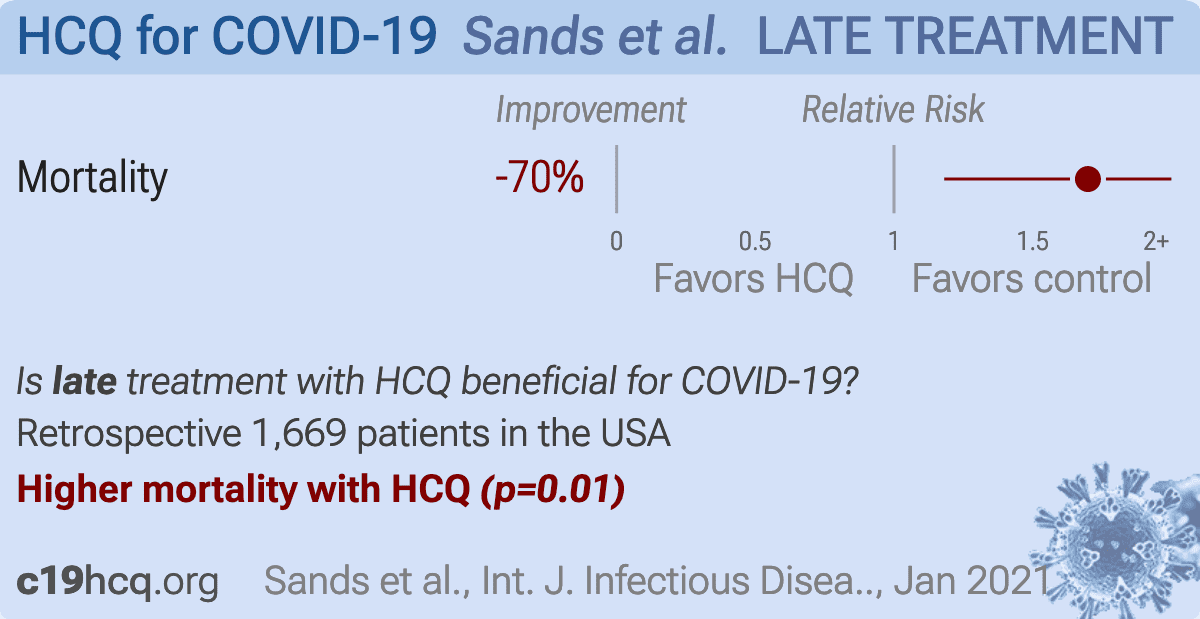
risk of death, 69.9% higher, RR 1.70, p = 0.01, treatment 101 of 973 (10.4%), control 56 of 696 (8.0%), odds ratio converted to relative risk.
|
|
Effect extraction follows pre-specified rules prioritizing more serious outcomes. Submit updates
|
Sands et al., 1 Jan 2021, retrospective, database analysis, USA, peer-reviewed, 10 authors.
No clinical benefit in mortality associated with hydroxychloroquine treatment in patients with COVID-19
Kenneth Sands, Richard Wenzel, Laura Mclean, Kimberly Korwek, Jonathon Roach, Karla Miller, Russell E Poland, L Hayley Burgess, Edmund Jackson, Jonathan B Perlin
International Journal of Infectious Diseases, doi:10.1016/j.ijid.2020.12.060
Background: The use of hydroxychloroquine (HCQ), with or without concurrent administration of azithromycin (AZM), for treatment of COVID-19 has received considerable attention. The purpose of this study was to determine whether HCQ administration is associated with improved mortality in COVID-19 patients. Methods: We conducted a retrospective analysis of data collected during the care process for COVID-19 positive patients discharged from facilities affiliated with a large healthcare system in the United States as of April 27, 2020. Patients were categorized by treatment with HCQ (in addition to standard supportive therapy) or receipt of supportive therapy with no HCQ. Patient outcomes were evaluated for in-hospital mortality. Patient demographics and clinical characteristics were accounted for through a multivariable regression analysis. Results: A total of 1669 patients were evaluated (no HCQ, n = 696; HCQ, n = 973). When adjusting for patient characteristics, receipt of AZM, and severity of disease at admission, there was no beneficial effect of receipt of HCQ on the risk of death. In this population, there was an 81% increase in the risk of mortality among patients who received HCQ at any time during their hospital stay versus no HCQ exposure (OR: 1.81, 95% CI: 1.20-2.77, p = 0.01). Conclusions: In this retrospective analysis, we found that there was no benefit of administration of HCQ on mortality in COVID-19 patients. These results support recent changes to clinical trials that discourage the use of HCQ in COVID-19 patients.
Conflict of interest The authors declare no conflicts interest.
Ethical approval This work was determined to be exempt from IRB oversight consistent with federal regulation and in accordance with institutional policy.
References
Bhimraj, Morgan, Shumaker, Lavergne, Baden et al., Infectious Diseases Society of America Guidelines on the Treatment and Management of Patients with COVID-19
Borba, Fda, Sampaio, Alexandre, Lacerda, Chloroquine diphosphate in two different dosages as adjunctive therapy of hospitalized patients with severe respiratory syndrome in the context of coronavirus (SARS-CoV-2) infection: Preliminary safety results of a randomized, double-blinded, phase IIb clinical trial (CloroCovid-19 Study), medRxiv,
doi:10.1101/2020.04.07.20056424Cavalcanti, Zampieri, Rosa, Azevedo, Veiga et al., Hydroxychloroquine with or without Azithromycin in Mild-to-Moderate Covid-19, New England Journal of Medicine,
doi:10.1056/NEJMoa2019014Chen, Zhou, Dong, Qu, Gong et al., Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: a descriptive study, Lancet,
doi:10.1016/s0140-6736(20)30211-7Clinicaltrials, Outcomes Related to COVID-19 Treated With Hydroxychloroquine Among In-patients With Symptomatic Disease (ORCHID)
Gautret, Lagier, Parola, Hoang, Meddeb et al., Clinical and microbiological effect of a combination of hydroxychloroquine and azithromycin in 80 COVID-19 patients with at least a six-day follow up: A pilot observational study, Travel Med Infect Dis,
doi:10.1016/j.tmaid.2020.101663Gautret, Lagier, Parola, Hoang, Meddeb et al., Hydroxychloroquine and azithromycin as a treatment of COVID-19: results of an open-label non-randomized clinical trial, Int J Antimicrob Agents,
doi:10.1016/j.ijantimicag.2020.105949Guy, Jackson, Perlin, Hernandez, Roman et al., Accelerating the Clinical Workflow Using the Sepsis Prediction and Optimization of Therapy (SPOT) Tool for Real-Time Clinical Monitoring, Ann Internal Med,
doi:10.7326/m20-2496%m32459529Keyaerts, Li, Vijgen, Rysman, Verbeeck et al., Antiviral Activity of Chloroquine against Human Coronavirus OC43 Infection in Newborn Mice, Antimicrob Agents Chemother,
doi:10.1128/aac.01509-08Li, Xu, Yu, Wang, Tao et al., Risk factors for severity and mortality in adult COVID-19 inpatients in Wuhan, J Allergy Clin Immunol,
doi:10.1016/j.jaci.2020.04.006Molina, Delaugerre, Goff, Lima, Ponscarme et al., No evidence of rapid antiviral clearance or clinical benefit with the combination of hydroxychloroquine and azithromycin in patients with severe COVID-19 infection, Médecine et Maladies Infectieuses,
doi:10.1016/j.medmal.2020.03.006Perinel, Launay, Botelho-Nevers, Diconne, Louf-Durier et al., Towards Optimization of Hydroxychloroquine Dosing in Intensive Care Unit COVID-19 Patients, Clin Infect Dis,
doi:10.1093/cid/ciaa394Richardson, Hirsch, Narasimhan, Crawford, Mcginn et al., Presenting Characteristics, Comorbidities, and Outcomes Among 5700 Patients Hospitalized With COVID-19 in the New York City Area, JAMA,
doi:10.1001/jama.2020.6775Ruan, Yang, Wang, Jiang, Song, Clinical predictors of mortality due to COVID-19 based on an analysis of data of 150 patients from Wuhan, China, Intens Care Med,
doi:10.1007/s00134-020-05991-xVincent, Bergeron, Benjannet, Erickson, Rollin et al., Chloroquine is a potent inhibitor of SARS coronavirus infection and spread, Virol J,
doi:10.1186/1743-422X-2-69Yao, Ye, Zhang, Cui, Huang et al., Vitro Antiviral Activity and Projection of Optimized Dosing Design of Hydroxychloroquine for the Treatment of Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2), Clin Infect Dis,
doi:10.1093/cid/ciaa237Zhou, Yu, Du, Fan, Liu et al., Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: a retrospective cohort study, Lancet,
doi:10.1016/S0140-6736(20)30566-3


{kind=link}