New insights into the antiviral effects of chloroquine
1st treatment shown to reduce risk in
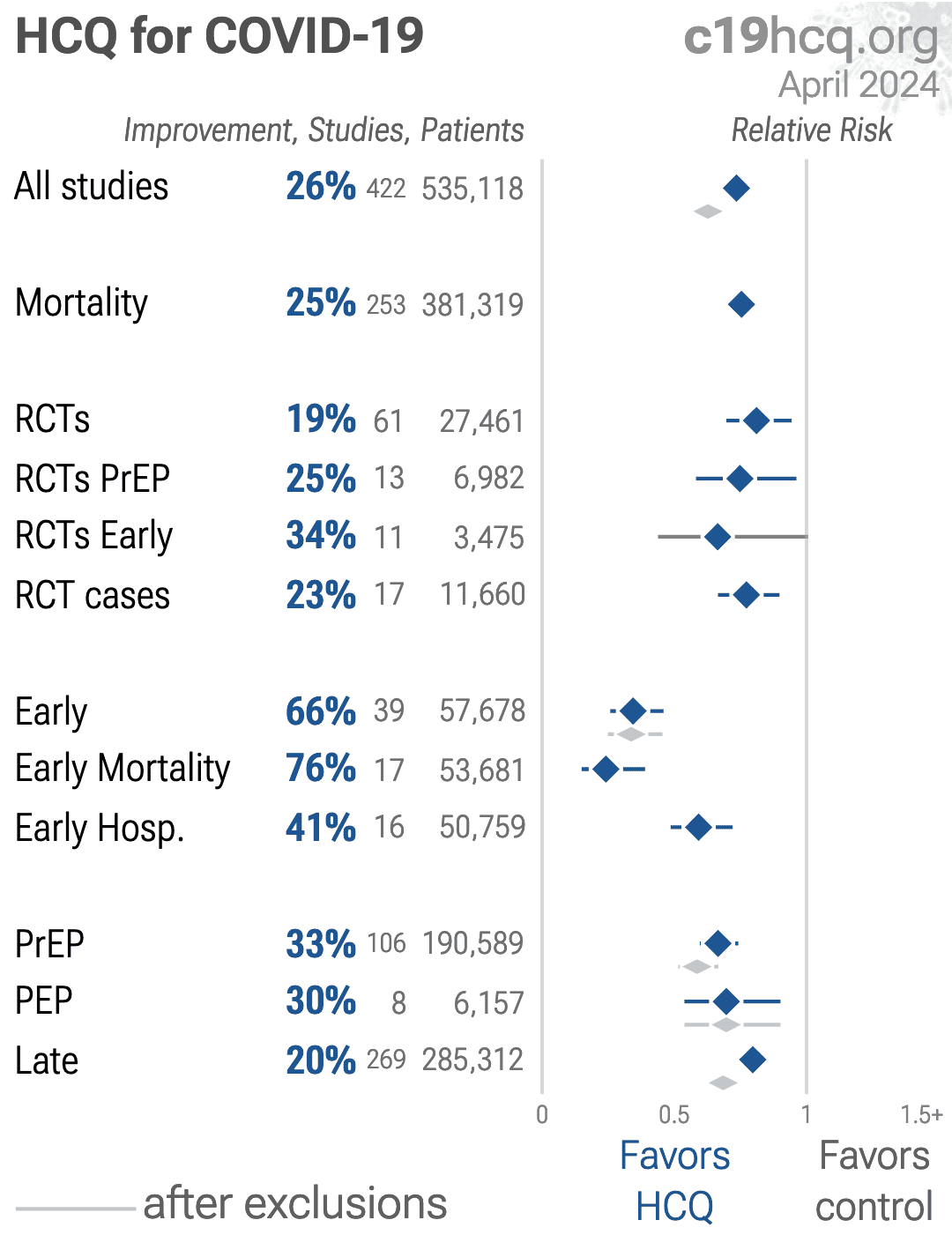
March 2020 *, now known with p < 0.00000000001 from 422 studies, recognized in 42 countries.
|
Update to 2003 paper. Hypothesis of CQ inhibiting SARS replication has been confirmed in two in-vitro studies. CQ affected an early stage of SARS replication.
31 preclinical studies support the efficacy of HCQ for COVID-19:
21 In Vitro studies Alsmadi, Andreani, Clementi, Dang, Delandre, Faísca, González-Paz, Kamga Kapchoup, Liu, Miao, Milan Bonotto, Mohd Abd Razak, Ou, Purwati, Shang, Sheaff, Wang, Wang (B), Wen, Yao, Yuan
Savarino et al., 1 Feb 2006, peer-reviewed, 5 authors.
In Vitro studies are an important part of preclinical research, however results may be very different in vivo.
Abstract: Reflection and Reaction
empirically, because of its activity against most of the
causative filamentous fungi and its time-tested
experience.7,8,10 Newer agents may be useful when
microbiological diagnosis is established (eg,
voriconazole for Aspergillus spp, posaconazole for
zygomycetes), although further studies are required.
Lastly, Van Damme and Hartman refer to noma
(chancrum oris), a devastating necrotising destructive
process of the face typically affecting young malnourished
children in Africa. This condition has been presented in a
recent excellent review by Baratti-Mayer and colleagues.14
We thank Van Damme and Hartman for their interest
in our paper, and their comments which allowed us to
elaborate upon the most important topic of rapidly
progressive SSTIs.
10
Donald C Vinh, John M Embil
11
DCV and JME are at the Section of Infectious Diseases,
Department of Medicine, University of Manitoba, Winnipeg,
Manitoba, Canada.
Correspondence to: Dr John Embil, Infection Prevention and
Control Unit, Health Sciences Centre, MS 673-820 Sherbrook
Street, Winnipeg, Manitoba, R3A 1R9, Canada. Tel +1 204 787
4654; fax +1 204 787 4699; jembil@hsc.mb.ca
1
2
3
4
5
6
7
8
9
12
13
14
Vinh DC, Embil JM. Rapidly progressive soft tissue infections.
Lancet Infect Dis 2005; 5: 501–13.
Djupesland PG. Necrotizing fasciitis of the head and neck—report of
three cases and review of the literature. Acta Otolaryngol 2000; 543
(suppl): 186–89.
Kimura AC, Pien FD. Head and neck cellulitis in hospitalized adults.
Am J Otolaryngol 1993; 14: 343–49.
Broadhurst LE, Erickson RL, Kelley PW. Decreases in invasive
Haemophilus influenzae diseases in US Army children, 1984 through
1991. JAMA 1993; 269: 227–31.
Givner LB. Periorbital versus orbital cellulitis. Pediatr Infect Dis J 2002;
21: 1157–58.
Lipsky BA, Berendt AR, Derry HG, et al. Infectious Diseases of America
guideline: diagnosing and treating diabetic foot infections. Clin Infect Dis
2004; 39: 885–910.
Johnson MA, Lyle G, Hanly M, et al. Aspergillus: a rare primary organism
in soft-tissue infections. Am Surg 1998; 64: 122–26.
Gettleman LK, Shetty AK, Prober CG. Posttraumatic invasive Aspergillus
fumigatus wound infection. Pediatr Infect Dis J 1999; 18: 745–47.
Sawyer RG, Schenk WG 3rd, Adams RB, et al. Aspergillus flavus wound
infection following repair of a ruptured duodenum in a nonimmunocompromised host. Scand J Infect Dis 1992; 24: 805–09.
Heinz T, Perfect J, Schell W, et al. Soft-tissue fungal infections: surgical
management of 12 immunocompromised patients. Plast Reconstr Surg
1996; 97: 1391–99.
Safdar A. Progressive cutaneous hyalohyphomycosis due to
Paecilomyces lilacinus: rapid response to treatment with caspofungin and
itraconazole. Clin Infect Dis 2002; 34: 1415–17.
Losee JE, Selber J, Vega S, et al. Primary cutaneous mucormycosis: guide
to surgical management. Ann Plast Surg 2002; 49: 385–90.
Andresen D, Donaldson A, Choo L, et al. Multifocal cutaneous
mucormycosis complicating polymicrobial wound infections in a
tsunami survivor from Sri Lanka. Lancet 2005; 365: 876–78.
Baratti-Mayer D, Pittet B, Montandon D, et al. Noma: an “infectious”
disease of unknown aetiology. Lancet Infect Dis 2003; 3: 419–31.
New insights into the antiviral effects of chloroquine
In a paper published 2 years ago in this journal, some of
us described the potentially therapeutic benefits of the
quinoline antimalarial chloroquine in viral diseases such
as HIV-1/AIDS and severe acute respiratory syndrome
(SARS).1..
Please send us corrections, updates, or comments.
c19early involves the extraction of 100,000+ datapoints from
thousands of papers.
Community updates
help ensure high accuracy.
Treatments and other interventions are complementary.
All practical, effective, and safe
means should be used based on risk/benefit analysis.
No treatment or intervention is 100% available and effective for all current
and future variants.
We do not provide medical advice. Before taking any medication,
consult a qualified physician who can provide personalized advice and details
of risks and benefits based on your medical history and situation.
FLCCC and
WCH
provide treatment protocols.
Submit

{kind=link}