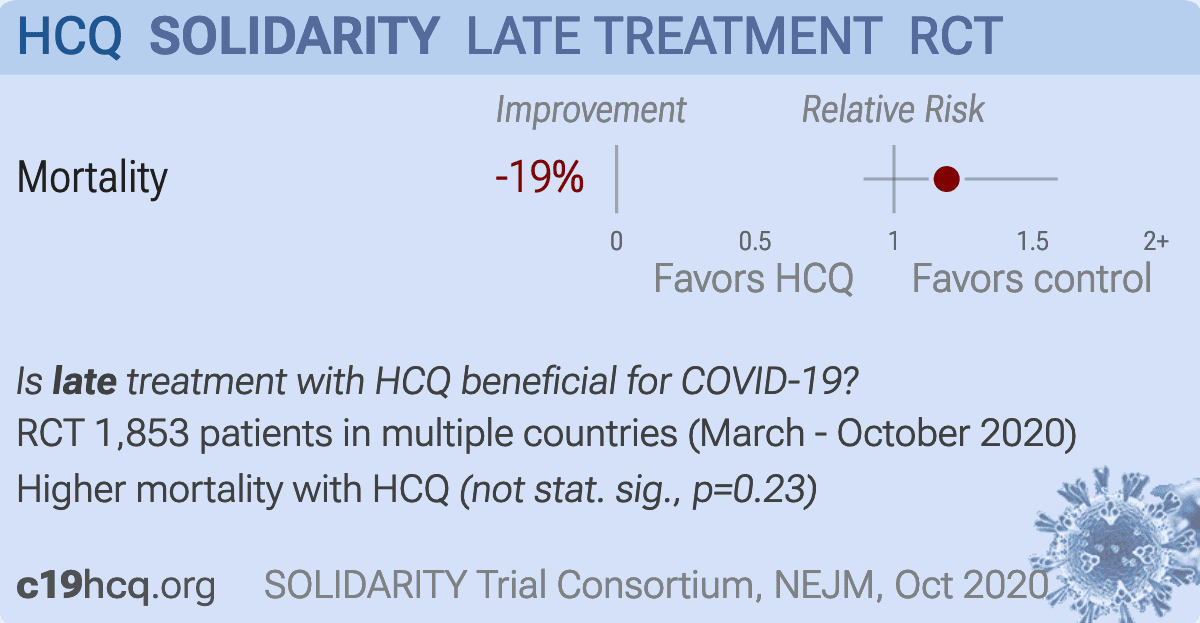
WHO SOLIDARITY open-label trial with 954 very late stage (64% on oxygen/ventilation) HCQ patients, mortality relative risk RR 1.19 [0.89-1.59], p=0.23.
HCQ dosage very high as in RECOVERY, 1.6g in the first 24 hours, 9.6g total over 10 days, only 25% less than the high dosage that Borba et al. show greatly increases risk (OR 2.8) Borba.
Authors state they do not know the weight or obesity status of patients to analyze toxicity (since they do not adjust dosage based on patient weight, toxicity may be higher in patients of lower weight).
KM curves show a spike in HCQ mortality days 5-7, corresponding to ~90% of the total excess seen at day 28 (a similar spike is seen in the RECOVERY trial).
Almost all excess mortality is from ventilated patients.
Authors refer to a lack of excess mortality in the first few days to suggest a lack of toxicity, but they are ignoring the very long half-life of HCQ and the dosing regimen - much higher levels of HCQ will be reached later. Increased mortality in Borba et al. occurred after 2 days.
An unspecified percentage used the more toxic CQ. No placebo used.
For more on the dosing problems see kristianfranciscomillanielsen.medium.com, also noting that concentrations vary substantially in different tissues and lung concentration may be >30x plasma concentration.
This study is excluded in the after exclusion results of meta
analysis:
excessive dosage in late stage patients, results do not apply to typical dosages; very late stage, >50% on oxygen/ventilation at baseline.
Abstract: medRxiv preprint doi: https://doi.org/10.1101/2020.10.15.20209817.this version posted October 15, 2020. The copyright holder for this preprint
(which was not certified by peer review) is the author/funder, who has granted medRxiv a license to display the preprint in perpetuity.
All rights reserved. No reuse allowed without permission.
1
MedRxiv (October 15) version
Repurposed antiviral drugs for COVID-19
–interim WHO SOLIDARITY trial results
WHO Solidarity trial consortium*
*A complete list of SOLIDARITY Trial investigators is
provided in the Supplementary Appendix.
Hongchao Pan, Ph.D., Richard Peto, F.R.S., Quarraisha Abdool Karim, Ph.D., Marissa Alejandria M.D., M.Sc., Ana Maria HenaoRestrepo, M.D., M.Sc., César Hernández García M.D., Ph.D., Marie-Paule Kieny Ph.D., Reza Malekzadeh M.D., Srinivas Murthy
M.D. C.M., Marie-Pierre Preziosi M.D., Ph.D., Srinath Reddy M.D., D.M., Mirta Roses Periago M. D., Vasee Sathiyamoorthy
B.M.B.Ch., Ph.D., John-Arne Røttingen M.D., Ph.D., and Soumya Swaminathan M.D. , as the members of the Writing Committee,
assume responsibility for the content and integrity of this article.
International Steering Committee *National PI; †National Coordinator; ‡Executive Group;§Discovery add-on study.
Albania: University Hospital Centre, Tirana N Como*; National Agency for Medicines and Medical Devices N Sinani†. Argentina:
Fundación del Centro de Estudios Infectológicos G Lopardo*; National Academy of Sciences of Buenos Aires M Roses Periago†‡.
Austria:§. Belgium:§. Brazil: Oswaldo Cruz Foundation EP Nunes*, PPS Reges†. Canada: University of British Columbia S
Murthy*‡; Public Health Agency of Canada M Salvadori†. Colombia: National University of Colombia CA Alvarez- Moreno*;
Ministry of Health ML Mesa Rubio†. Egypt: National Hepatology and Tropical Medicine Research Institute M Hassany*; Ministry of
Health and population H Zaid†. Finland: Helsinki University Hospital and South Karelian Central Hospital, Lappeenranta KAO
Tikkinen*; Finnish Institute for Health and Welfare and University of Finland, Helsinki M Perola†. France: Hospices Civils de Lyon,
Lyon F Ader*§; Institut National de la Santé Et de la Recherche Médicale, Paris MP Kieny†‡§. Honduras: National Autonomous
University of Honduras MT Medina*; Secretaria de Salud de Honduras N Cerrato†. India: ICMR National AIDS Research Institute,
Pune S Godbole*†; Public Health Foundation of India KS Reddy‡. Indonesia: National Institute of Health Research and
Development I Irmansyah*; RSUP Persahabatan, Jakarta MR Rasmin†. Iran (Islamic Republic of): Digestive Disease Research
Institute, Teheran University of Medical Sciences, Tehran R Malekzadeh*†‡. Ireland: HRB Clinical Research Facility, University
College, Cork J Eustace*; Department of Health T Maguire†. Italy: University of Verona E Tacconelli*; Italian Medicines Agency N
Magrini†. Kuwait: Infectious Diseases Hospital A Alhasawi*; Ministry of Health A Al-Bader†. Lebanon: Rafic Hariri University
Hospital P Abi Hanna*; Ministry of Public Health R Hamra†. Luxembourg:§. Lithuania: University Hospital Santaros klinikos,
Vilnius L Jancoriene*, L Griskevicius†. Malaysia: Penang Hospital TS Chow*; Hospital Sungai Buloh, Jalan Hospital S Kumar†.
North Macedonia: University Clinic of Infectious Diseases and Febrile Conditions M Stevanovikj*; Ministry of Health S
Manevska†. Norway: Oslo University Hospital P Aukrust*, A Barratt-Due†; Research Council of Norway JA Røttingen‡. Pakistan:
Shaukat Khanum Memorial Cancer..
Late treatment is less effective
Please send us corrections, updates, or comments.
c19early involves the extraction of 100,000+ datapoints from
thousands of papers. Community updates
help ensure high accuracy.
Treatments and other interventions are complementary.
All practical, effective, and safe
means should be used based on risk/benefit analysis.
No treatment or intervention is 100% available and effective for all current
and future variants.
We do not provide medical advice. Before taking any medication,
consult a qualified physician who can provide personalized advice and details
of risks and benefits based on your medical history and situation. FLCCC and WCH
provide treatment protocols.


{kind=link}