The role of organizational characteristics on the outcome of COVID-19 patients admitted to the ICU in Belgium
Fabio Silvio Taccone, Nina Van Goethem, Robby De Pauw, Xavier Wittebole, Koen Blot, Herman Van Oyen, Tinne Lernout, Marion Montourcy, Geert Meyfroidt, Dominique Van Beckhoven
The Lancet Regional Health - Europe, doi:10.1016/j.lanepe.2020.100019
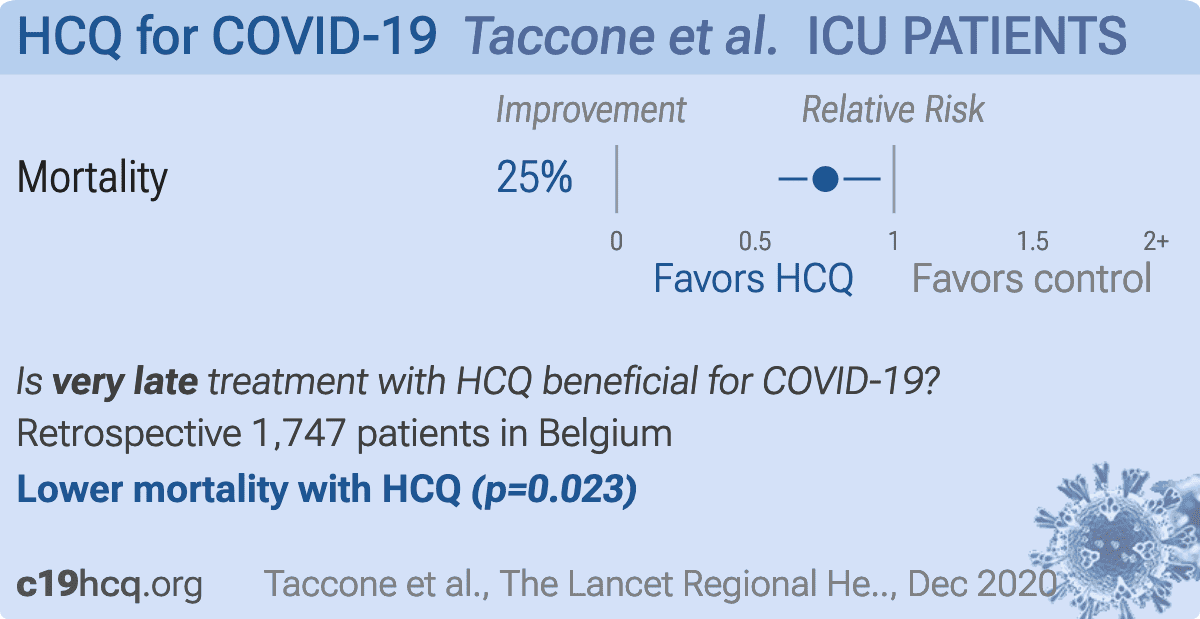
Background: Several studies have investigated the predictors of in-hospital mortality for COVID-19 patients who need to be admitted to the Intensive Care Unit (ICU). However, no data on the role of organizational issues on patients' outcome are available in this setting. The aim of this study was therefore to assess the role of surge capacity organisation on the outcome of critically ill COVID-19 patients admitted to ICUs in Belgium. Methods: We conducted a retrospective analysis of in-hospital mortality in Belgian ICU COVID-19 patients via the national surveillance database. Non-survivors at hospital discharge were compared to survivors using multivariable mixed effects logistic regression analysis. Specific analyses including only patients with invasive ventilation were performed. To assess surge capacity, data were merged with administrative information on the type of hospital, the baseline number of recognized ICU beds, the number of supplementary beds specifically created for COVID-19 ICU care and the "ICU overflow" (i.e. a time-varying ratio between the number of occupied ICU beds by confirmed and suspected COVID-19 patients divided by the number of recognized ICU beds reserved for COVID-19 patients; ICU overflow was present when this ratio is 1.0). Findings: Over a total of 13,612 hospitalised COVID-19 patients with admission and discharge forms registered in the surveillance period (March, 1 to August, 9 2020), 1903 (14.0%) required ICU admission, of whom 1747 had available outcome data. Non-survivors (n = 632, 36.1%) were older and had more frequently various comorbid diseases than survivors. In the multivariable analysis, ICU overflow, together with older age, presence of comorbidities, shorter delay between symptom onset and hospital admission, absence of hydroxychloroquine therapy and use of invasive mechanical ventilation and of ECMO, was independently associated with an increased in-hospital mortality. Similar results were found in in in the subgroup of invasively ventilated patients. In addition, the proportion of supplementary beds specifically created for COVID-19 ICU care to the previously existing total number of ICU beds was associated with increased in-hospital mortality among invasively ventilated patients. The model also indicated a significant between-hospital difference in in-hospital mortality, not explained by the available patients and hospital characteristics. Interpretation: Surge capacity organisation as reflected by ICU overflow or the creation of COVID-19 specific supplementary ICU beds were found to negatively impact ICU patient outcomes.
Authors' contributions FST, NVG and DVB conceived the study; NVG, RDP and KB selected the population; NVG, MM, RDP and KB reviewed all available data; NVG, RDP, KB, HVO, TL and MM conducted the statistical analysis; FST, GM, NVG and DVB and wrote the first draft of the paper; XW, KB, HVO, TL and MM revised the text for intellectual content. All the authors have full access to the data of the present study, approved the final version of this manuscript and accepted responsibility to submit for publication. NVG, GM and DVB has verified the data of the study.
Declaration of Competing Interests FST received lecture fees from BD, Zoll, Nihon Khoden and Neuroptics, which are all outside the content of the present study. Other authors declare that they have no competing interests.
Ethics approval and consent to participate The hospital data collection performed by Sciensano, the Belgian Institute of Public Health, is legally entitled for surveillance of infectious diseases in Belgium (Royal Decree of 21/03/2018). The COVID-19 clinical surveillance was authorized by an independent administrative authority protecting privacy and personal data, and approved by the ethical committee of Ghent University Hospital (BC-07507).
Funding
No funding was obtained to this study
Supplementary materials Supplementary material associated with this article can be found, in the online version, at doi:10.1016/j.lanepe.2020.100019.
References
Aziz, Arabi, Alhazzani, Managing ICU surge during the COVID-19 crisis: rapid guidelines, Intensive Care Med
Azoulay, De Waele, Ferrer, Symptoms of burnout in intensive care unit specialists facing the COVID-19 outbreak, Ann Intensive Care
Azoulay, Fartoukh, Darmon, Increased mortality in patients with severe SARS-CoV-2 infection admitted within seven days of disease onset, Intensive Care Med
Catteau, Dauby, Montourcy, Low-dose hydroxychloroquine therapy and mortality in hospitalised patients with COVID-19: a nationwide observational study of 8075 participants, Int J Antimicrob Agents
Cummings, Baldwin, Abrams, Epidemiology, clinical course, and outcomes of critically ill adults with COVID-19 in New York City: a prospective cohort study, Lancet
Fiolet, Guihur, Rebeaud, Effect of hydroxychloroquine with or without azithromycin on the mortality of coronavirus disease 2019 (COVID-19) patients: a systematic review and meta-analysis, Clin Microbiol Infect,
doi:10.1016/j.cmi.2020.08.022Gattinoni, Chiumello, Caironi, COVID-19 pneumonia: different respiratory treatments for different phenotypes?, Intensive Care Med
Grasselli, Greco, Zanella, Risk Factors associated with mortality among patients With COVID-19 in intensive care units in Lombardy, Italy, JAMA Intern Med
Grasselli, Pesenti, Cecconi, Critical care utilization for the COVID-19 outbreak in Lombardy, Italy: early experience and forecast during an emergency response, JAMA
Grasselli, Tonetti, Protti, Pathophysiology of COVID-19-associated acute respiratory distress syndrome: a multicentre prospective observational study, Lancet Respir Med
Grasselli, Zangrillo, Zanella, Baseline characteristics and outcomes of 1591 patients infected with SARS-CoV-2 admitted to ICUs of the Lombardy region, Italy, JAMA
Haase, Plovsing, Christensen, Characteristics, interventions and longerterm outcomes of COVID-19 ICU patients in Denmark -a nationwide, observational study, Acta Anaesthesiol Scand,
doi:10.1111/aas.13701Karagiannidis, Mostert, Hentschker, Case characteristics, resource use, and outcomes of 10 021 patients with COVID-19 admitted to 920 German hospitals: an observational study, Lancet Respir Med
Lagier, Million, Gautret, Outcomes of 3,737 COVID-19 patients treated with hydroxychloroquine/azithromycin and other regimens in Marseille, France: a retrospective analysis, Travel Med Infect Dis
Malgie, Schoones, Pijls, Decreased mortality in COVID-19 patients treated with Tocilizumab: a rapid systematic review and meta-analysis of observational studies, Clin Infect Dis,
doi:10.1093/cid/ciaa1445Qian, Alaa, Van Der Schaar, Ercole, Between-centre differences for COVID-19 ICU mortality from early data in England, Intensive Care Med
Recovery Collaborative Group, Horby, Lim, Emberson, Dexamethasone in hospitalized patients with Covid-19 -preliminary report, N Engl J Med,
doi:10.1056/NEJMoa2021436Recovery Collaborative Group, Horby, Mafham, Linsell, Effect of hydroxychloroquine in hospitalized patients with Covid-19, N Engl J Med,
doi:10.1056/NEJMoa2022926Remuzzi, Remuzzi, COVID-19 and Italy: what next?, Lancet
Rhodes, Ferdinande, Flaatten, Guidet, Metnitz et al., The variability of critical care bed numbers in Europe, Intensive Care Med
Richardson, Hirsch, Narasimhan, Presenting characteristics, comorbidities, and outcomes among 5700 patients hospitalized with COVID-19 in the New York city area, JAMA
Sanders, Monogue, Jodlowski, Cutrell, Pharmacologic treatments for coronavirus disease 2019 (COVID-19): a review, JAMA,
doi:10.1001/jama.2020.6019Schmidt, Hajage, Lebreton, Extracorporeal membrane oxygenation for severe acute respiratory distress syndrome associated with COVID-19: a retrospective cohort study, Lancet Respir Med
Van Goethem, Vilain, Wyndham-Thomas, Rapid establishment of a national surveillance of COVID-19 hospitalizations in Belgium, Arch Public Health
Wang, Hu, Hu, Clinical characteristics of 138 hospitalized patients with 2019 novel coronavirus-infected pneumonia in Wuhan, China, JAMA
Xu, Yang, Yang, Clinical course and predictors of 60-day mortality in 239 critically ill patients with COVID-19: a multicenter retrospective study from Wuhan, China, Crit Care
Yang, Yu, Xu, Clinical course and outcomes of critically ill patients with SARS-CoV-2 pneumonia in Wuhan, China: a single-centered, retrospective, observational study, Lancet Respir Med,
doi:10.1016/S2213-2600(20)30079-5


{kind=link}