Risk factors for mortality in hospitalized patients with COVID-19 at the start of the pandemic in Belgium: a retrospective cohort study
Karlijn Van Halem, Robin Bruyndonckx, Jeroen Van Der Hilst, Janneke Cox, Paulien Driesen, Matthias Opsomer, Eveline Van Steenkiste, Björn Stessel, Jasperina Dubois, Peter Messiaen
BMC Infectious Diseases, doi:10.1186/s12879-020-05605-3
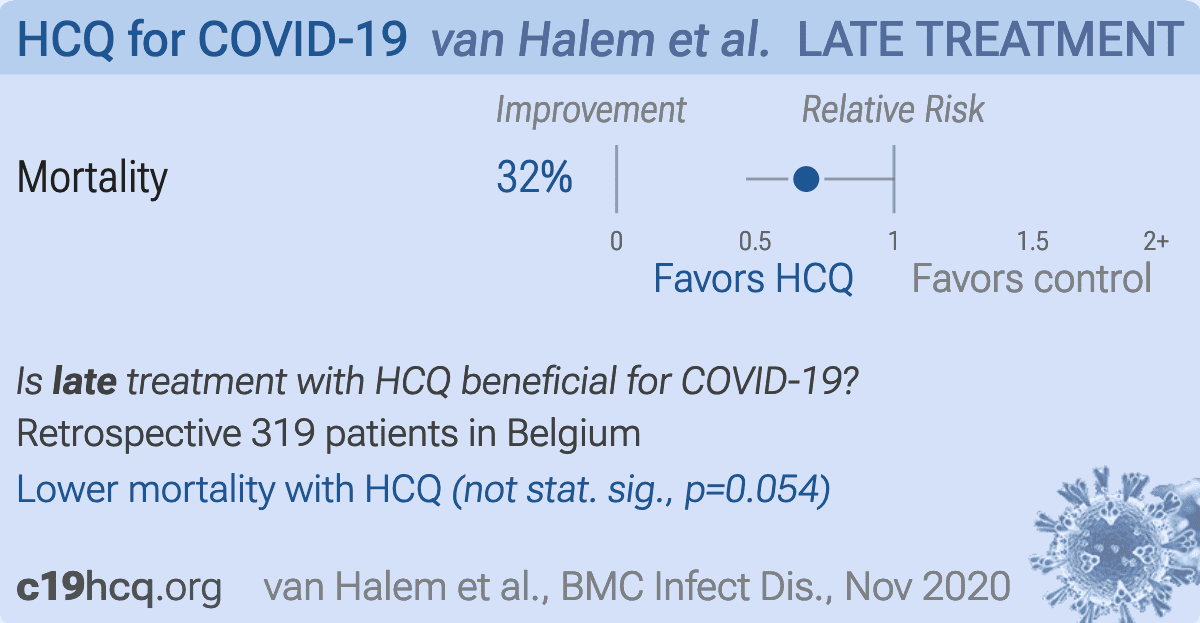
Background: Belgium was among the first countries in Europe with confirmed coronavirus disease 2019 cases. Since the first diagnosis on February 3rd, the epidemic has quickly evolved, with Belgium at the crossroads of Europe, being one of the hardest hit countries. Although risk factors for severe disease in COVID-19 patients have been described in Chinese and United States (US) cohorts, good quality studies reporting on clinical characteristics, risk factors and outcome of European COVID-19 patients are still scarce. Methods: This study describes the clinical characteristics, complications and outcomes of 319 hospitalized COVID-19 patients, admitted to a tertiary care center at the start of the pandemic in Belgium, and aims to identify the main risk factors for in-hospital mortality in a European context using univariate and multivariate logistic regression analysis. Results: Most patients were male (60%), the median age was 74 (IQR 61-83) and 20% of patients were admitted to the intensive care unit, of whom 63% needed invasive mechanical ventilation. The overall case fatality rate was 25%. The best predictors of in-hospital mortality in multivariate analysis were older age, and renal insufficiency, higher lactate dehydrogenase and thrombocytopenia. Patients admitted early in the epidemic had a higher mortality compared to patients admitted later in the epidemic. In univariate analysis, patients with obesity did have an overall increased risk of death, while overweight on the other hand showed a trend towards lower mortality. Conclusions: Most patients hospitalized with COVID-19 during the first weeks of the epidemic in Belgium were admitted with severe disease and the overall case fatality rate was high. The identified risk factors for mortality are not easily amenable at short term, underscoring the lasting need of effective therapeutic and preventative measures.
Supplementary Information The online version contains supplementary material available at https://doi. org/10.1186/s12879-020-05605-3. Additional file 1: Table S1
Ethics approval and consent to participate The study was approved by the Ethics Committee of Jessa Hospital, Hasselt, Belgium (ethical approval number 20.38-infect20.06). The requirement for informed consent was waived because of the retrospective nature of the study.
Consent for publication Not applicable.
Competing interests The authors declare that they have no competing interests.
Publisher's Note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
Beigel, Tomashek, Dodd, Mehta, Zingman et al., ACTT-1 Study Group Members. Remdesivir for the Treatment of Covid-19 -Final Report, N Engl J Med,
doi:10.1056/NEJMoa2007764Cavalcanti, Zampieri, Rosa, Azevedo, Veiga et al., Coalition Covid-19 Brazil I Investigators. Hydroxychloroquine with or without Azithromycin in Mild-to-Moderate Covid-19, N Engl J Med,
doi:10.1056/NEJMoa2019014Firth, Bias reduction of maximum likelihood estimates, Biometrika
Fu, Wang, Yuan, Chen, Ao et al., Clinical characteristics of coronavirus disease 2019 (COVID-19) in China: A systematic review and meta-analysis, J Infect,
doi:10.1016/j.jinf.2020.03.041Geleris, Sun, Platt, Zucker, Baldwin et al., Observational study of Hydroxychloroquine in hospitalized patients with Covid-19, N Engl J Med
Giacomelli, Ridolfo, Milazzo, Oreni, Bernacchia et al., 30-day mortality in patients hospitalized with COVID-19 during the first wave of the Italian epidemic: a prospective cohort study, Pharmacol Res
Grasselli, Zangrillo, Zanella, Antonelli, Cabrini et al., Baseline Characteristics and Outcomes of 1591 Patients Infected With SARS-CoV-2 Admitted to ICUs of the Lombardy Region, Italy, JAMA,
doi:10.1001/jama.2020.5394Ji, Zhang, Xu, Chen, Yang et al., Prediction for Progression Risk in Patients With COVID-19 Pneumonia: The CALL Score, Clin Infect Dis,
doi:10.1093/cid/ciaa414Klok, Kruip, Van Der Meer, Arbous, Gommers et al., Incidence of thrombotic complications in critically ill ICU patients with COVID-19, Thromb Res
Lighter, Phillips, Hochman, Sterling, Johnson et al., Obesity in Patients Younger Than 60 Years Is a Risk Factor for COVID-19 Hospital Admission, Clin Infect Dis,
doi:10.1093/cid/ciaa415Middeldorp, Coppens, Van Haaps, Foppen, Vlaar et al., Incidence of venous thromboembolism in hospitalized patients with COVID-19, J Thromb Haemost,
doi:10.1111/jth.14888Nie, Zhang, Jee, Jung, Li et al., Obesity survival paradox in pneumonia: a meta-analysis, BMC Med
Petrilli, Jones, Yang, Rajagopalan, Donnell et al., Factors associated with hospital admission and critical illness among 5279 people with coronavirus disease 2019 in New York City: prospective cohort study, Bmj
Recovery Collaborative Group, Horby, Lim, Emberson, Mafham et al., Dexamethasone in Hospitalized Patients with Covid-19 -Preliminary Report, N Engl J Med,
doi:10.1056/NEJMoa2021436Richardson, Hirsch, Narasimhan, Crawford, Mcginn et al., Presenting Characteristics, Comorbidities, and Outcomes Among 5700 Patients Hospitalized With COVID-19 in the New York City Area, JAMA,
doi:10.1001/jama.2020.6775Rosenberg, Dufort, Udo, Wilberschied, Kumar et al., Association of Treatment with Hydroxychloroquine or azithromycin with inhospital mortality in patients with COVID-19 in New York state, Jama
Rubin, Multiple Imputation for Nonresponse in Surveys
Schetz, Jong, Deane, Druml, Hemelaar et al., Obesity in the critically ill: a narrative review, Intensive Care Med
Sciensano, COVID 19 epidemiologisch bulletin
Sciensano, Interim clinical guidance for adults with suspected or confirmed COVID-19 in Belgium
Simonnet, Chetboun, Poissy, Raverdy, Noulette et al., High prevalence of obesity in severe acute respiratory syndrome Coronavirus-2 (SARS-CoV-2) requiring invasive mechanical ventilation, Obesity (Silver Spring)
Stapleton, Dixon, Parsons, Ware, Suratt, The association between BMI and plasma cytokine levels in patients with acute lung injury, Chest
Stefan, Birkenfeld, Schulze, Ludwig, Obesity and impaired metabolic health in patients with COVID-19, Nat Rev Endocrinol
Stessel, Vanvuchelen, Bruckers, Geebelen, Callebaut et al., Impact of implementation of an individualised thromboprophylaxis protocol in critically ill ICU patients with COVID-19: a longitudinal controlled before-after study, Thromb Res
Tomlins, Hamilton, Gunning, Sheehy, Moran et al., Clinical features of 95 sequential hospitalised patients with novel coronavirus 2019 disease (COVID-19), the first UK cohort, J Infect,
doi:10.1016/j.jinf.2020.04.020Van Buuren, Multiple imputation of discrete and continuous data by fully conditional specification, Stat Methods Med Res
Van Halem, Cox, Messiaen, Pat, Declercq et al., Care for adult non-ICU Covid-19 patients: early experiences from a Belgian tertiary care Centre, Neth J Med
Who, Management of COVID-19 Interim guidance
Wu, Liu, Zhao, Liu, Wang, Clinical characteristics of imported cases of coronavirus disease 2019 (COVID-19) in Jiangsu Province: a multicenter descriptive study, Clin Infect Dis


{kind=link}