HCQ+AZ adjusted death HR 0.44, p=0.009. Propensity scores include baseline COVID-19 disease severity, age, gender, number of comorbidities, cardio-vascular disease, duration of symptoms, date of admission, baseline plasma CRP. IPW censoring. Retrospective study of 539 COVID-19 hospitalized patients in Milan, with treatment a median of 1 day after admission. HCQ 197 patients, HCQ+AZ 94, control 92. Control group received various other treatments. Authors excluded people receiving other drugs which could have biased the effect of HCQ when used in combination. Residual confounding is possible (e.g., people with CVD were more frequent in control), however people in the control group were more likely to require mechanical ventilation.
|
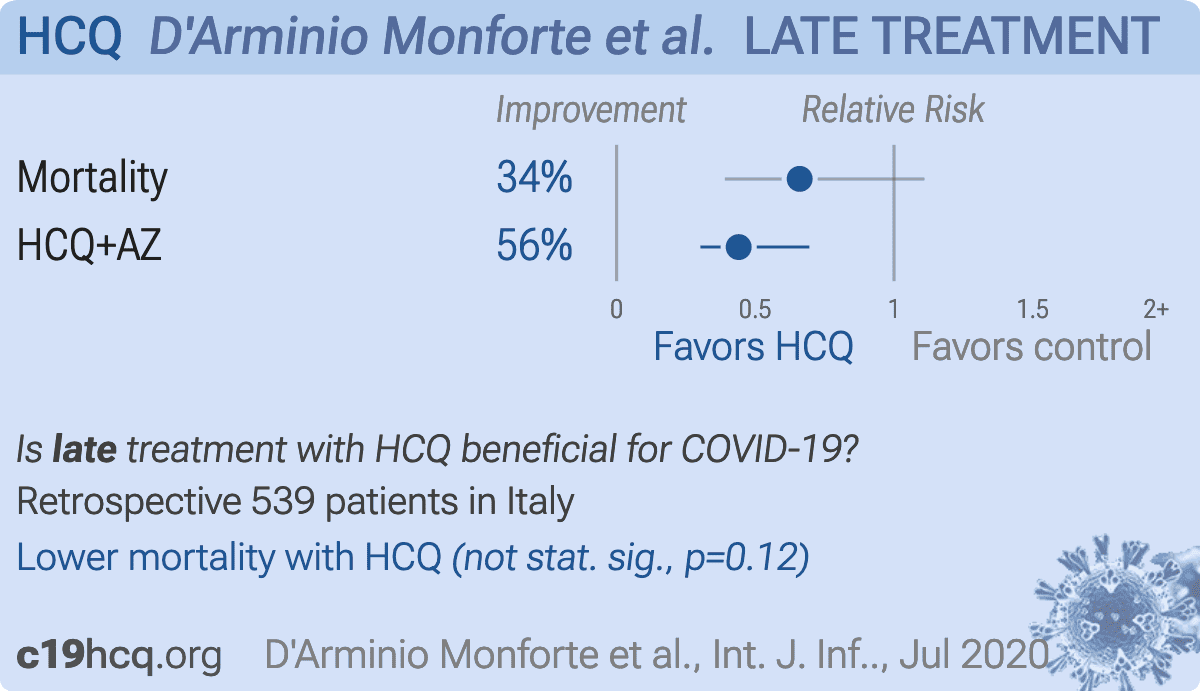
risk of death, 34.0% lower, HR 0.66, p = 0.12, treatment 53 of 197 (26.9%), control 47 of 92 (51.1%), NNT 4.1, adjusted per study.
|
|
HCQ+AZ, 56.0% lower, HR 0.44, p = 0.009, treatment 22 of 94 (23.4%), control 47 of 92 (51.1%), NNT 3.6, adjusted per study.
|
|
Effect extraction follows pre-specified rules prioritizing more serious outcomes. Submit updates
|
D'Arminio Monforte et al., 29 Jul 2020, retrospective, Italy, peer-reviewed, 5 authors.
Effectiveness of hydroxychloroquine in COVID-19 disease: A done and dusted deal?
Antonella D’arminio Monforte, Alessandro Tavelli, Francesca Bai, Giulia Marchetti, Alessandro Cozzi-Lepri
International Journal of Infectious Diseases, doi:10.1016/j.ijid.2020.07.056
A total of 539 COVID-19 hospitalized patients were included in our cohort in Milan, from February 24 to May 17, 2020, of whom 174 died in hospital (day 14 probability of death: 29.5% -95%CI: 25.5-34.0). We divided a subset of our cohort into three groups who started treatment a median of 1 day after admission: those receiving hydroxychloroquine alone (N = 197), those receiving hydroxycholoroquine + azithromycin (N = 94), and those receiving neither (controls) (N = 92). Of the latter group, ten started HIV antivirals (boosted-lopinavir or -darunavir), one teicoplanin, twelve immunomodulatory drugs, or corticosteroids, 23 heparin and 46 remained untreated. The percent of death in the three groups was 27%, 23%, and 51%. Mechanical ventilation was used in 4.3% of hydroxychloroquine, 14.2% of hydroxychloroquine + azithromycin, and 26.1% of controls. Unweighted and weighted relative hazards of mortality are shown in Table 1 . After adjusting * Adjusted for age, gender, number of comorbidities, CVD (yes/no), duration of symptoms, date of admission, CRP and censoring using IPW. £ The overall estimate was also adjusted for baseline COVID-19 disease severity. # Heparin, immuno-modulatory drugs, HIV antivirals, combinations of these or no drugs at all. & 45 patients missing baseline PO2/FiO2 not included in the stratified analysis.
Declarations of interest None declared.
Ethical approval This analysis is part of the study approved by Ethic Committee Area 1, Milan Italy (2020/ST/049 and 2020/ST/049_BIS, 11/03/ 2020).
References
Arshad, Kigore, Chaudhry, Jacobsen, Wang et al., Treatment with hydroxychloroquine, azithromycin, and combination in patients hospitalised with COVID-19, Int J Infect Dis,
doi:10.1016/j.ijid.2020.06.09Devaux, Rolain, Colson, Raoult, New insights on the antiviral effects of chloroquine against coronavirus: what to expect for COVID-19?, Int J Antimicrob Agents,
doi:10.1016/j.antimicag.2020.105938Gautret, Lagier, Parola, Hoang, Meddeb et al., Hydroxychloroquine and azithromycin as a treatment of COVID-19: results of an open-label non-randomised clinical trial, Int J Antimicrob Agents,
doi:10.1016/j.antimicag.2020.105949Geleris, Sun, Platt, Zucker, Baldwin et al., Observational study on hydroxychloroquine in hospitalized patients with COVID-19, N Engl J Med,
doi:10.1056/NEJMoa2012410Horby, Lim, Emberson, Mafham, Bell et al., Effect of desamethasone in hospitalized patients with CVID-19: preliminary report
Lee, Mackenzie, Mcdonald, Tong, An observational cohort study of hydroxychloroquine and azithromycin for COVID-19: (Can't get no) satisfaction, Int J Infect Dis,
doi:10.1016/j.ijid.2020.06.095Liu, Cao, Xu, Wang, Zhang et al., Hydroxychloroquine, a less toxic derivative of chloroquine, is effective in inhibiting SARS-CoV-2 infection in vitro, Cell Discov
Tang, Cao, Han, Wang, Chen et al., Hydroxychloroquine in patients mainly with mild to moderate COVID-19: an open-label, randomised, controlled trial, BMJ,
doi:10.1136/bmj.m1849


{kind=link}